ECR 2018 / C-1905
Intracranial Epidermoids- Benign lesion,Interesting locations but difficult solutions
Congress:
ECR 2018
Poster Number:
C-1905
Type:
Educational Exhibit
Keywords:
Cysts, Imaging sequences, MR, CNS
Authors:
S. Arooj1, S. Kadri2, S. Sheikh1, S. Hamid3; 1Karachi/PK, 2Karachi, karachi/PK, 3Karachi, Sindh/PK
DOI:
10.1594/ecr2018/C-1905

Fig. 1:
35 years old man with history of trauma and headache; T1WI show cystic lesion...

Fig. 3:
Same patient, no post contrast enhancement is noted.

Fig. 4:
Same patient, diffusion restriction seen in the lesion

Fig. 2:
Same patient, Minimally expansile lesion in occipital horn left lateral...

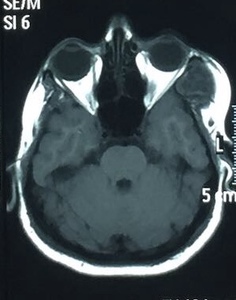
Fig. 5:
34 year old man with syncope; T1W hypointense area in fourth ventricle

Fig. 6:
34 year old man with syncope; T2W hyperintense area in fourth ventricle

Fig. 7:
34 year old man with syncope; diffusion restriction is seen in fourth ventricle

Fig. 8:
34 year old man with syncope; diffusion restriction is seen in fourth ventricle

Fig. 9:
34 year old man with syncope; heterogenous FLAIR signals in fourth ventricle

Fig. 10:
30 year old man with swelling lateral aspect of left eye since birth;...

Fig. 11:
same patient; hyperintense T2W signals lateral canthus left eye

Fig. 12:
Same patient, no enhancement is seen on post gadolinium T1WI.

Fig. 13:
Same patient, diffusion restriction is seen on DWI

Fig. 14:
Post gadolinium T1WI show no significant enhancement.

Fig. 15:
33 year old patient with extra axial intracranial epidermoid hyperintense on...

Fig. 16:
33 year old patient with extra axial intracranial epidermoid hypointense on...

Fig. 17:
33 year old patient with extra axial intracranial epidermoid shows diffusion...

Fig. 18:
15 years old patient with ill defined Hypointense area on T1WI

Fig. 19:
15 years old patient with ill defined Hyperintense area on T2WI

Fig. 20:
15 years old patient with ill defined heterogenous area on FLAIR

Fig. 21:
15 years old patient with ill defined area in basal cisterns which shows...

Fig. 22:
15 years old patient with ill defined area in basal cisterns which shows...

Fig. 23:
10 year old girl with history of frontal headache shows T2W hyperintense area...

Fig. 24:
same patient, same lesion appears hypointense on T1WI

Fig. 25:
Same lesion appears heterogenous on FLAIR images

Fig. 26:
Same lesion shows diffusion restriction on DWI