The term PID includes inflammation of the uterus,
fallopian tubes and ovaries and is a common cause of abdominal pain in young women.
PID has significant acute and chronic morbidity and associated financial implications.
In the UK,
latest figures put the diagnosis of PID in 16-44 year olds at 176/100,000 in the general practice setting and 241/100,00 in the hospital setting per year (2011) [1,
2].
PID diagnosis rates were most frequent in the 20-24 year old age group within the general practice (GP) setting but hospital diagnosis of PID tend to occur in an older age group of 35-44 years old.
While recent analysis shows that rates of diagnosis are declining in the GP setting,
hospital diagnosis rates remain stable [2].
PID may be (Fig. 1):
- Primary (originating from gynaecological tract)
- Secondary
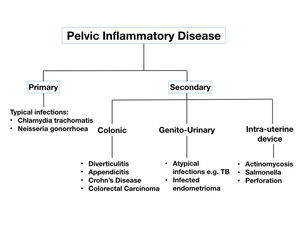
Fig. 1: Flow diagram of causes of primary and secondary pelvic inflammatory disease
Primary PID
Primary causes of PID tend to occur in younger sexually active patients through sexually transmitted speed of infectious organisms such as;
- Chlamydia trachomatis,
- Mycoplasma genitalium,
- Neisseria gonorrhoeae.
Less that <15% of cases are caused by:
- Streptococci,
- Staphylococci,
- H.
Influenza,
- E.
Coli as well as other gastrointestinal flora.
Many patients (approximately 30-40%) will have a polymicrobial infection of several organisms [3,
4].
Risk factor for the development of primary PID include young age of first intercourse,
new partner in the last 3 months,
multiple sexual partners and previous sexually transmitted diseases.
Instrumentation,
such as hysteroscopy,
hysterosalpingogram (HSG),
insertion of an intrauterine device,
termination of pregnancy or IVF can also cause spread of organisms from the vagina tract into the uterus and peritoneum [3].
In primary PID,
the causative organisms often infect the vagina before spreading to the cervix,
endometrium and uterus and then via the fallopian tubes to the ovaries and peritoneal cavity.
In the acute setting,
primary PID causes cervicitis,
endometritis and salpingitis and can develop into pyosalpinx or tubo-ovarian abscess (TOA).
In later stages,
complications such as Fitz Hugh Curtis syndrome,
infertility,
ectopic pregnancy,
adhesions and peritoneal inclusion cysts.
Secondary PID
Secondary causes of PID tend to occur in young patients without a history of sexual intercourse or older,
often post-menopausal,
patients.
Many of these infections arise in other adjacent organs and include inflammatory bowel diseases,
appendicitis and perforated or locally advanced colonic cancer.
In a recent study,
female patients with Crohn’s disease had a greater risk of ectopic pregnancy,
which was further increased after bowel related surgery and independent of co-existent primary PID or endometriosis [5].
Rarer infections can also develop such as tuberculosis and actinomycosis.
Symptoms of PID can be similar for both primary and secondary causes and include:
- Bilateral lower abdominal pain,
- Vaginal discharge,
- Dyspareunia,
- Bleeding - often inter-menstrual or post-coital.
Most cases of PID are diagnosed based on clinical history,
examination and vaginal swabs.
The 2011 UK national PID guideline states that PID diagnosis should be considered if “recent onset,
bilateral lower abdominal pain associated with local tenderness on bimanual vaginal examination,
in whom pregnancy has been excluded” [1].
However,
the presentation of PID may be subtle or atypical giving rise to multiple differential diagnoses which require further investigation with imaging.
Ultrasound is the primary imaging modality,
but in the acute setting when the diagnosis is broad,
CT may be preferred.
Chronic cases or complications can be investigated with US,
MRI and hysterosalpingogram.

