Moya-moya disease:
Described in the English literature by Japanese neurosurgeons in the 1960's,
moya-myoa disease (MMD) is a chronic,
occlusive cerebrovascular disease characterized by progressive stenosis at the terminal portion of the internal carotid artery (ICA) and an abnormal vascular network at the base of the brain [1]. The term “moyamoya” is derived from a Japanese expression for something hazy,
like a puff of cigarette smoke drifting in the air.
The diagnostic criteria [1],
from 1997, proposed by the Research Committee on Spontaneous Occlusion of the Circle of Willis suggested three principal factors as follows:
- Stenosis or occlusion at the terminal portion of the internal carotid artery (ICA) and/or at the proximal portion of the anterior and/or middle cerebral arteries;
- Abnormal vascular networks in the vicinity of the occlusive or stenotic lesions in the arterial phase;
- Lesion bilaterality.
Recently,
in 2015, statement by the Research Committee of MMD of the Japanese Ministry of Health,
Labour and Welfare [2],
proposed the key modification that the “bilaterality” was omitted.
If unilateral disease is observed,
a cerebral angiography is needed to confirm the diagnosis, whereas bilateral cases can be promptly diagnosed by either catheter angiography or magnetic resonance imaging/angiography (MRI/MRA) [2].
So,
is there a place for ultrasound to monitored MMD?
Yes, particularly Power doppler,
as it is more sensitive to detect low-velocity blood flow signals in arteries that appeared occluded on cerebral angiography [3].
Patient 1:
A 11-year-old boy who had a right hemispheric ischemic stroke when he was only 10-months-old.
When he was 14-month-old,
he had another ischemic event,
involving his left hemisphere,
resulting in a right-sided hemiparesis.
During the investigation,
a MMD was confirmed on a cerebral angiography (not shown).
Fig.1,
shows a TOF-MRA before and after he underwent revascularization surgery,
in 2011,
with good collateralization results after it.
The transcranial doppler ultrasound (TCD),
Fig.2 confirmed left middle cerebral artery (MCA) patency and,
in some patients,
this method may be more sensitive detecting arterial flow than MRA.
Vertebral artery dissection in a patient with fibromuscular dysplasia
A dissection is produced by subintimal penetration of blood in a vessel with subsequent longitudinal extension of the intramural hematoma for a varying distance between its layers,
and it is usually associated with an intimal tear [4].
Although vertebrobasilar and intracranial carotid dissections are less common,
than the extracranial carotid artery, with the advance in imaging techniques,
asymptomatic multiple vessel involvement can be detected [5]. Cervicocephalic arterial dissections have been reported after trivial trauma [4] and it has been is also associated with fibromuscular dysplasia, connective tissue disease such as Marfan's syndrome and Ehlers-Danlos syndrome [5],
and moyamoya disease.
The traditional method for visualization of arterial dissection is cerebral angiography. MR images can show a periarterial rim of intramural hematoma typically show hyper intense signal on T1 and T2 weighted images. The reported sensitivity of neurovascular ultrasound for detecting spontaneous arterial dissection varies from 80 to 96% [5].
As for fibromuscular dysplasia (FMD),
it is a non-atheromatous, non-inflammatory arteriopathy of unknown etiology with segmental manifestation on medium-sized arteries in various regions of the body [6].
Second to the renal arteries in prevalence [7],
extracranial cervical FMD, especially the ICA are attacked,
often bilaterally but manifestation also occurs on the vertebral artery (VA) [6].
Depending on the type of FMD (intimal, medial,
and subadventitial-perimedial), ultrasound findings correlate with the angiographic findings,
and may show segmental narrowing and widening or the color flow in cervical arteries,
with the characteristic string of beads appearance in medial type of FMD,
long tubular stenosis,
usually distally from a widened carotid bulb in intimal type of FMD,
or irregular local widening of the arterial wall in subadventitial type of FMD [5].
Patient 2:
A 44-year-old female patient presenting a cervical pain and a right hemiparesis,
after physical exercise.
The CT-angiophaphy and MRI (DWI and ADC map) Fig.
3,
showed an acute ischemic stroke in the dorsal lateral in medulla oblongata on the right side.
The color doppler ultrasound,
Fig.4 showed different blood flow velocities in the vertebral arteries,
with lower velocity on the right.
The carotid color and power doppler ultrasound examination, Fig.5, revealed wall irregularities,
with bilateral kinking of both ICAs.
The cerebral angiography,
Fig.6 confirmed the CT-angiography and ultrasound findings of right vertebral dissection (B+C) and marked wall irregularities,
with areas of stenosis followed by dilatation in the more distal right ICA (A) - compatible with FMD.
Takayasu's arteritis
Takayasu’s arteritis (TA) is an idiopathic granulomatous vasculitis that affects the aortic arch and its main branches with unknown etiology [8]. Most patients are young women [9]. It has three stages [5]:
- Systemic stage,
with symptoms and signs of an active inflammatory illness dominate;
- Vascular inflammatory stage,
when stenosis,
aneurysms,
and vascular pain tend to occur.
This stage sometimes overlaps with the systemic stage;
- Burned-out stage develops when fibrosis sets in,
and this stage is usually associated with remission.
Although it is difficult to establish the diagnosis in the early stages,
ultrasound can help identify early TA.
Cerebral angiography is a gold standard [5],
and it shows changes in the lumen in many arteries.
Sonography shows changes mainly of the arterial wall in a small number of important arteries,
as delineated characteristic long segments with homogeneous,
midechoic,
circumferential arterial wall thickening,
which has been described as the ‘macaroni sign’ [9].
Sonography and cerebral angiography are complementary methods in the diagnosis of Takayasu arteritis.
Patient 3:
A 15-year-old female patient diagnosed with TA when she was 11-year-old,
after episodes of severe headache and multiple episodes of transient ischemic accidents with left sided hemiparesis and dysarthria.
During the hospital stay she underwent several complementary diagnostic examinations: the carotid ultrasound discovered mural thickening on both common carotid arteries with partial luminal obliteration and low flow velocities,
Fig.7.
These findings were confirmed by MRA,
with marked stenosis and occlusion of large vessels,
Fig.
8.
Giant cell arteritis
Giant cell arteritis (GCA),
is also known as temporal arteritis or cranial arteritis,
is the most common form of vasculitis that occurs in adults,
older than the age of 50.
It is a granulomas arteritis affecting large or medium sized artery,
usually temporal or ophthalmic artery [5].
It can be considered an ophthalmological emergency, its most serious complication being irreversible visual acuity loss secondary to ischemic optic neuropathy that may become bilateral within a few days or weeks if a prompt diagnosis and treatment are not established [10]. Standard test for diagnosing GCA is biopsy of the temporal artery [5]. In recent years,
non-invasive imaging techniques such as color doppler ultrasound have been applied to overcome the limitations of the biopsy. Temporal artery color doppler ultrasound is able to identify three characteristic ultrasound features [10]:
- A periluminal hypoechogenic halo reflecting arterial wall edema;
- Segmental arterial stenosis
- Arterial luminal occlusion in severe cases.
A positive halo sign strongly supports a diagnosis of GCA in the presence of compatible clinical manifestations,
but the absence of a halo does not rule it out [11].
This sign is due to vessel wall edema and can be distinguished from the focal hyperechoic wall thickening seen in atherosclerosis [12]. During healing regression of the dark halo will be visible parallel with the restitution of the color coded flow [5].
Patient 4:
A 72-year-old female patient with a history of jaw claudication,
was admitted in the emergency room due to posterior circulation ischemic stroke (Fig.9)- with prostration,
walk imbalance and nausea.
During the hospital stay,
the ultrasound (Fig.10) revealed thickening / “halo sign” on both vertebral and superficial temporal arteries.
The CT-angiography confirmed the vertebral arteries (VA) findings (Fig.11).
Her erythrocyte sedimentation rate was elevated and a GCA was considered.
She started methylprednisolone with improvement of symptoms.
Sickle cell disease
Children with sickle cell disease (SCD) are at high risk for stroke. The risk is highest in children with elevated blood flow velocity in the distal internal carotid terminal internal carotid artery or proximal middle cerebral artery (MCA),
as measured with transcranial doppler ultrasound (TCD)[13].
Chronic blood transfusions,
if implemented in a timely fashion in those with flow velocity >200 cm/s,
can reduce the risk of stroke by as much as 92%.
It is also suggested that unilateral high-flow velocity indicates stenosis,
whereas bilateral high-velocity represents bilateral stenosis,
hyperemia,
or both [14].
It is important to emphasize that the STOP velocity criteria apply only to children with SCD who have not had a stroke.
Those with abnormal velocity should undergo repeated screening within the next few weeks and if the second study is also abnormal should be offered transfusion therapy [15].
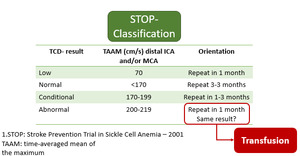
Fig. 14
References: Nichols, F. et al; American Society of Neuroimaging (2001)
Patient 5:
A 17-year-old female patient,
diagnosed at 1year of age with sickle cell disease after several vaso-occlusive crises.
Under a regular regime of blood transfusions since 2013.
Due to important cerebral vasculopathy (bilateral ischemic lesions and a right ICA stenosis),
she was submitted to an indirect brain revascularization (encephalo-duro-arterio-synangiosis) in 2014,
with good vascular results - Fig.12.
On Fig.13 you can see the TCD showing high velocities on the left MCA and a regularization of the blood flow,
after surgery.
Radiation induced vasculopathy
Cerebral arteriopathy may result from therapeutic irradiation of neck or intracranial malignancies such as lymphoma,
thyroid cancer,
or glioma.
The vascular complications usually develop 6 months to 10 years after irradiation [8].
It is an underrecognized precursor to ischemic stroke [16] in these patients. In children,
and rarely in adults,
it may be associated with the formation of netlike vessels and transdural anastomoses (moyamoya disease). The exact pathogenesis of radiation-induced carotid artery disease is still unclear [17] and the literature is quite unclear on this matter. Some authors have argued that chronic occlusive radiation vasculopathy is primarily an accelerated form of atherosclerosis; others have described it as a distinct disease entity shaped by the initial radiation insult to the vasa vasorum [16].
A hallmark of radiation vasculopathy is its occurrence in patients who lack traditional vascular risk factors. The diagnosis of carotid stenosis still relies principally on the imaging approaches [17].
Patient 6
A 65-year-old man patient,
with a history of larynx cancer,
treated with surgery and radiation,
had a wake-up stroke with left sided hemiparesis.
Brain-CT showed a right insular and external capsule infarct - Fig 14.
During the hospital stay,
he underwent vascular study with carotid ultrasound that showed hyperechoic infiltration on both carotid axis,
with an occluded right CCA and VA,
and a > 50% stenosis on left ICA most likely related with neck radiation performed 12 years-ago.
Both the cerebral angiography and CT-angiography confirmed these findings,
Fig. 15.


 reveals patency of both middle cerebral arteries (MCA)")
.
C+D: DWI+ADC map showed a restricted diffusion area in the right dorsolateral medulla oblongata - an acute ischemic stroke.")



 - blue asterisk.
Using Oower doppler (B+D) note the weak luminal filling, indicating stenosis.")

B: TOF-MRA: circle of willis (3D)
Note the vessels asymmetry. Intracranial circulation is mainly dependent on the right vertebral artery (blue arrow).")
, ADC map (B) confirmed the acute ischemic lesion involving the pontine tegmentum bilaterally and also the right middle cerebellar peduncle.
FLAIR (C) showing the same lesions (blue arrows).")
 of the right TSA, corresponding to wall artery thickening due to wall oedema.")

 before (A) and after (B) the revascularization surgery.
Note the anatomic variant: left VA fenestration.")
 and after (B+D) the indirect revascularization surgery.
Note the regularization of arterial velocity flow on the left MCA.")

Note no color mode filling nor flux registered either in the right common carotid artery (B) and vertebral artery (C).")
; divides into inferior thyroid artery (blue arrow) and ascending cervical artery ( red arrow). Also note the deep cervical artery (yellow arrow).
B: CT-angiography - 3D")