Keywords:
Abdomen, Oncology, Pancreas, MR, Diagnostic procedure
Authors:
L. Bertuzzo1, G. A. Zamboni1, L. Mannelli2, R. Negrelli1, R. Pozzi-Mucelli1; 1Verona/IT, 2New York, NY/US
DOI:
10.1594/ecr2018/C-2027
Methods and materials
IRB approval was not required for this retrospective study,
which was conducted according to the Declaration of Helsinki,
and informed consent was waived.
Patient population
From a search on the PACS system of our hospital to identify patients with IPMN who underwent a MRI/MRCP with Gadolinium at our Institution,
we selected 56 consecutive patients.
The study population included 22 males and 34 females with an average age at the time of the examination of 67.4 years.
MRI imaging
MRI examinations were performed using two 1.5 Tesla systems: MAGNETOM® Symphony (Siemens,
Erlangen,
Germany) and Ingenia (Philips Medical System,
Eindhoven,
Netherlands).
Respectively a 4-channel coil and a 32-channel coil were placed over the upper abdomen.
All patients were required to fast for 4-6 hours prior to the examination.
In order to cancel the signal from the gastroduodenal fluid on the T2-weighted sequences,
200 ml of pineapple juice were administered before the investigation.
No antiperistaltic agent was administered.
The sequence protocol included: axial and coronal T2-weighted and axial T1- weighted sequences with and without fat saturation centered on the upper abdomen,
2D and 3D MRCP sequences including the entire biliary tree and the pancreatic ductal system,
and a dynamic study with T1- weighted volumetric fat sat sequences during the administration of 0.1 mmol/kg of body weight of gadolinium chelates (Multihance,
Bracco,
Milan,
Italy) at a rate of 2.5 ml/s with quadriphasic technique followed by 15–25 ml of saline solution: pre-contrast,
pancreatic (35–45 s),
portal venous (85–90 s),
and late phase (>180 s).
MRI protocol technical parameters are synthetized in the following tables.
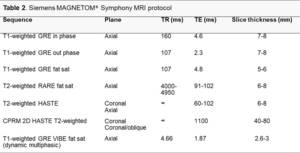
Fig. 1: Siemens MAGNETOM MRI protocol
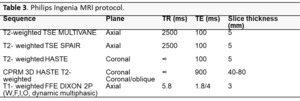
Fig. 2: Philips Ingenia MRI protocol
Image analysis
Two readers each with more than 10 years’ experience in abdominal imaging,
working in two referral centers for pancreatic disease,
reviewed independently the scans assessing for:
- walls and internal septa thickening
- solid mural nodules
- MPD dilation
- walls and internal septa enhancement
- mural nodules enhancement.
Readers were blinded to clinical/laboratory information.
Kappa statistics was calculated.
