Anonymized abdominal radiographs were retrieved from case collections and submitted for review.
The following cases demonstrate the utility of plain radiography in foreign body evaluation.
MATERIALS IDENTIFIED ON RADIOGRAPHS
A variety of materials can be detected using radiography,
but some are easier to identify than others.
It is important to know what various materials look like on radiographs to avoid missing important findings.
Metal is very radiopaque,
and easily detected on plain radiographs (Figure 1).
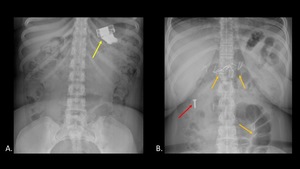
Fig. 1: AP abdominal radiographs (A,B) demonstrate foreign bodies composed of metal, including batteries (yellow arrow), nails (orange arrows), and a screw (red arrow).
Plastic is more difficult to detect due to its radiolucency (Figure 2). Some plastic objects such as the pen and toothbrush shown have radiopaque components which aid in detection.
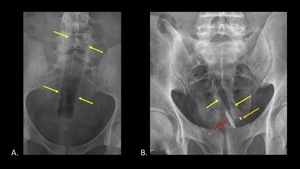
Fig. 2: AP abdominal radiographs demonstrate plastic foreign bodies which were inserted rectally. A travel toothbrush case (A) (yellow arrows) is almost completely radiolucent, and is identified by the presence of straight lines in the body and air within the tube. A pen and toothbrush (B) inserted next to one another are more easily identified due to the presence of radiopaque components, such as the tip of the pen (orange arrow) and tongue scraper on the toothbrush (red arrow). The plastic components are radiolucent (yellow arrows).
Organic material such as wood or other plant-based material can be very difficult to detect (Figure 3).
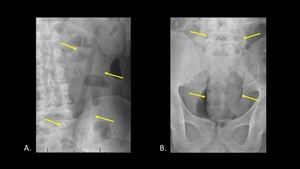
Fig. 3: AP abdominal radiographs demonstrate the appearance of organic material on x-ray, including wood (A) and plant-based material (B). Both foreign bodies are indicated with yellow arrows.
The presence of straight lines and unusual contours can be helpful for detecting foreign bodies composed of organic material.
ROUTES OF ENTRY
There are several potential routes of entry for foreign bodies:
-Ingestion (oral)
-Insertion (rectal,
vaginal,
urethral,
transcutaneous,
through ostomy)
-Iatrogenic (migration or erosion of surgically implanted objects,
retained surgical instruments)
FOREIGN BODY INGESTION
Ingestion of foreign bodies is commonly seen in the pediatric population,
but can also be encountered in adults who accidentally swallow items,
or who suffer from dementia or mental health problems.
It is important for the emergency radiologist to recognize ingested foreign bodies early,
because some swallowed items such as batteries,
magnets or sharp objects may pose unique risks to the patient.
Small,
inert objects often pass through the GI tract without complication.
These may be monitored with serial radiographs (Figure 4).
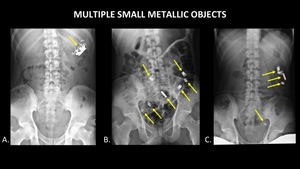
Fig. 4: Serial AP abdominal radiographs demonstrate the passage of multiple small metallic foreign bodies (yellow arrows) though the GI tract, from the stomach (A), to the small bowel (B), and large bowel (C).
Larger objects may require endoscopic or surgical removal (Figure 5).

Fig. 5: AP abdominal radiograph demonstrates a metallic spoon (yellow arrow) in the stomach.
Some swallowed materials are difficult to detect,
such as these pencil fragments (Figure 6).
The straight contours and lead within the broken pencil aid in identification.
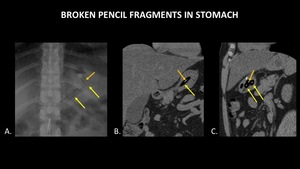
Fig. 6: AP abdominal radiograph (A), coronal abdominal CT (B), and sagittal abdominal CT (C) demonstrate fragments of a broken pencil within the stomach (yellow arrows). Radiopaque lead (orange arrows) within the pencil fragments aids in foreign body detection on both plain radiograph and CT. The wooden portion of the pencil is radiolucent, with a density similar to air.
Certain swallowed foreign bodies require special attention due to the risk of complications.
Magnets pose a special risk to patients when more than one is swallowed,
because they can be attracted to one another inside the body,
leading to obstruction,
bowel necrosis and even death.
Neodymium magnets are powerful magnets which have been swallowed by many children.
In this instance,
the magnets were attracted to one another in the stomach (Figure 7).
These could not all be removed endoscopically,
and open surgery was ultimately required.
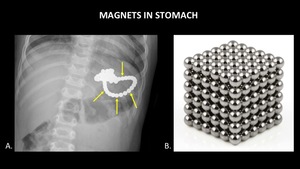
Fig. 7: AP abdominal radiograph (A) demonstrates multiple round magnets (yellow arrows) within the stomach of a child. A photograph (B) of a block made of this type of magnet is provided for reference.
Some patients suffer from a compulsion to swallow sharp objects.
Commonly swallowed items include tacks,
nails,
screws and razor blades.
Sharp objects pose a risk to patients because they can perforate the bowel.
In some instances,
the objects may puncture the bowel and enter the peritoneal space without causing pneumoperitoneum or acute abdomen (Figure 8).
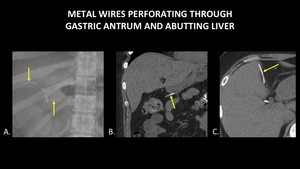
Fig. 8: AP abdominal radiograph (A) demonstrates two thin, curvilinear densities in the right upper quadrant (yellow arrows), one of which projects over cholecystectomy clips. Coronal abdominal CT (B) demonstrates a thin, metallic foreign body (yellow arrow) perforating through the gastric antrum. Axial abdominal CT (C) demonstrates a thin, metallic foreign body (yellow arrow) within the peritoneal cavity, abutting the liver. In this case, there is no free air or fat stranding, and the patient did not demonstrate signs of peritonitis.
Swallowed drug packets pose a unique risk,
as they can rupture and cause an overdose.
To identify drug packets on a plain radiograph,
look for multiple densities within the bowel which are uniform in shape and size (Figure 9).
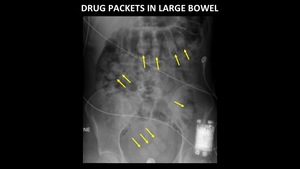
Fig. 9: AP abdominal radiograph demonstrates multiple drug packets (yellow arrows) in the large bowel. Note the uniform shape, size and density of the objects.
Some patients who suffer from mental illness will present to the emergency department on multiple occasions,
having swallowed a variety of objects (Figure 10).
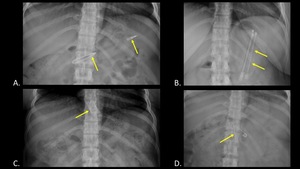
Fig. 10: AP abdominal radiographs of the same patient taken on different dates demonstrate a variety of swallowed foreign bodies (yellow arrows), including a pen (A), springs (B), a razor blade (C), and open safety pin (D).
The use of plain radiography allows rapid,
accurate,
cost-effective identification of foreign bodies while limiting the lifetime radiation dose to those who require frequent imaging.
FOREIGN BODY INSERTION
Foreign bodies may be inserted via several routes,
including rectal,
vaginal,
urethral and transcutaneous.
While most inserted foreign bodies will cause no significant complication,
it is important for the emergency radiologist to be aware of the most common associated pathology,
including bowel perforation and damage to adjacent structures.
The following cases demonstrate the utility of plain films for detecting inserted foreign bodies and identifying complications.
RECTALLY INSERTED FOREIGN BODIES
Figure 11 demonstrates a pen and toothbrush lying parallel to one another in the rectosigmoid colon.
These plastic objects would be very difficult to identify without the radiopaque components,
namely the tip of the pen and the tongue scraper.
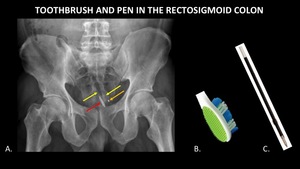
Fig. 11: AP abdominal radiograph (A) demonstrates a toothbrush and pen (yellow arrows) in the rectosigmoid colon. These objects are almost entirely radiolucent, but radiopaque components including the tongue scraper on the toothbrush (red arrow) and tip of the pen (orange arrow) aid in detection. Photographs (B, C) of a similar toothbrush and pen refill are included for reference.
Figure 12 demonstrates a travel toothbrush case in the rectum.
This object is more difficult to identity because it is made entirely of plastic,
which is relatively radiolucent.
The presence of straight contours and air within the tube aid in identifying the foreign body.
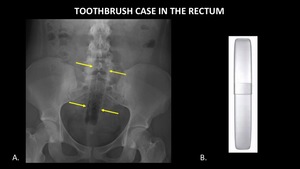
Fig. 12: AP abdominal radiograph (A) demonstrates a plastic travel toothbrush case (yellow arrows) in the rectum. The object is relatively radiolucent, but more easily detected due to its straight contours and the air it contains. A photograph (B) of a similar toothbrush case is provided for reference.
Figure 13 demonstrates an aerosol can in the rectum.
The object is easily identified because it is made of metal.
The contents of the can are radiolucent,
consistent with air.
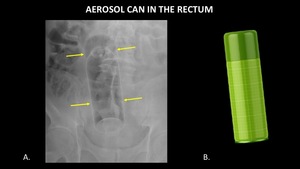
Fig. 13: AP abdominal radiograph (A) demonstrates an aerosol can (yellow arrows) in the rectum. A photograph (B) of a similar can is included for reference.
Figure 14 demonstrates an electronic device in the rectum. It is easily identified because of its metallic components and batteries.
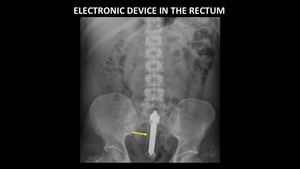
Fig. 14: AP abdominal radiograph demonstrates an electronic device (yellow arrow) in the rectum.
Figure 15 demonstrates a silicone object in the form of male genitalia in the rectum.
While not as radiopaque as metal,
this object is still relatively easy to identify on radiographs due to its high density.
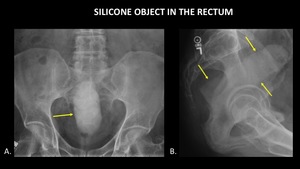
Fig. 15: AP abdominal radiograph (A) and Sagittal radiograph (B) of the pelvis demonstrate a silicone object (yellow arrows) in the form of male genitalia in the rectum.
Figure 16 demonstrates a cucumber in the rectosigmoid colon.
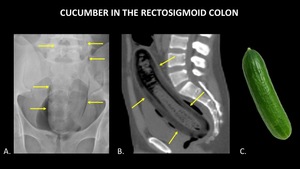
Fig. 16: AP abdominal radiograph (A) and sagittal abdominal CT (B) demonstrate a cucumber (yellow arrows) in the rectosigmoid colon. A photograph (C) of a cucumber is included for reference.
Although the foreign body is large,
it is difficult to identify on plain radiographs because the density is very similar to soft tissue.
This is true for a variety of organic materials.
Looking for unusual contours within the body can be very helpful for identifying such objects.
In this case,
the object is better defined on computed tomography.
COMPLICATIONS RELATED TO RECALLY INSERTED FOREIGN BODIES
Most rectally inserted foreign bodies will not cause complications,
likely because the rectosigmoid bowel is naturally well lubricated,
capacious and able to dilate.
However,
one of the most common complications is bowel perforation,
so the emergency radiologist should always look for free air on plain radiographs.
Figure 17 demonstrates a wooden rolling pin in the rectosigmoid colon,
and free air under the diaphragm indicating bowel perforation.
It is important to identify pneumoperitoneum early,
because the patient will require surgical exploration.
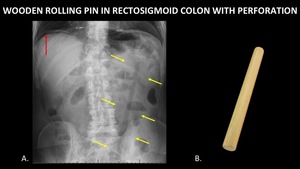
Fig. 17: AP abdominal radiograph (A) demonstrates a wooden rolling pin (yellow arrows) in the rectosigmoid colon. This was complicated by bowel perforation, as evinced by free air under the diaphragm (red arrow). A photograph (B) of a similar rolling pin is included for reference.
Like the cucumber,
the rolling pin demonstrates a density very similar to soft tissue.
However,
it is relatively easy to detect because of the straight lines it creates,
which are not seen on normal radiographs.
Figure 18 demonstrates a light bulb in the rectum,
and air surrounding the kidneys on both plain film and CT.
This is a unique example of pneumoretroperitoneum due to bowel perforation.
Note that the diagnosis can be made on the plain radiographs.
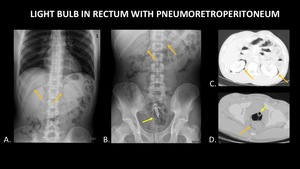
Fig. 18: AP abdominal radiographs (A, B) demonstrate a light bulb (yellow arrow) in the rectum, and air (orange arrows) in the retroperitoneum surrounding the kidneys. Axial CT (C, D) again demonstrates the light bulb in the rectum (yellow arrow) and confirms pneumoretroperitoneum (orange arrows).
Injury to adjacent organs is also possible,
although not readily seen on plain radiographs.
When advanced imaging is obtained,
one must critically assess adjacent organs for evidence of injury.
Figure 19 demonstrates a small shampoo bottle in the rectum. While no obvious complication is identified on the plain radiograph,
the CT demonstrates an enlarged,
edematous left seminal vesicle.
This most likely represents an injury related to trauma from foreign body insertion.
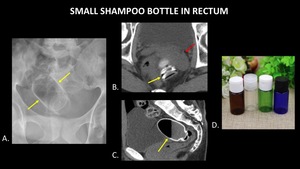
Fig. 19: AP abdominal radiograph (A) demonstrates a small shampoo bottle (yellow arrows) in the rectum. Axial abdominal CT (B) demonstrates the bottle (yellow arrow) in the rectum, abutting an enlarged, edematous left seminal vesicle (red arrow). Trace free fluid was also present in the pelvis (not pictured). Findings are consistent with left seminal vesicle injury due to trauma from foreign body insertion. Sagittal abdominal CT (C) demonstrates the partially filled bottle (yellow) in the rectum, with an air fluid level in the bottle. A photograph (D) of a similar type of bottle is included for reference.
This case demonstrates an important limitation of plain radiography.
Serious injury may be present,
but not visible on plain radiographs.
Advanced imaging should be obtained if the clinical presentation warrants further investigation.
VAGINALLY INSERTED FOREIGN BODIES
Although relatively uncommon,
some patients may present with foreign bodies in the vagina.
Complications are uncommon,
but can include mucosal irritation or perforation.
Figure 20 demonstrates a deformed bra underwire in the vagina which was inserted by the patient.
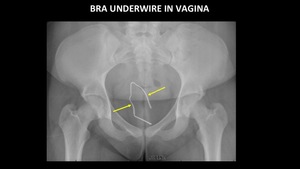
Fig. 20: AP abdominal radiograph demonstrates a deformed bra underwire (yellow arrows) in the vagina.
URETHRAL FOREIGN BODIES
Urethral foreign bodies are more commonly reported in males than females.
While individuals insert objects into the urethra for a variety of reasons,
this is most commonly associated with psychiatric disorders,
intoxication and autoerotic stimulation.
Plain radiographs serve as a valuable first line test for identifying urethral foreign bodies.
More advanced imaging studies such as the retrograde urethrogram are required to diagnose urethral injury,
and will not be covered.
Figure 21 demonstrates a pencil in the male urethra.
The pencil is more easily identified because of the straight contour and increased opacity of the lead.
The wood is radiolucent.

Fig. 21: AP abdominal radiograph demonstrates a pencil (yellow arrows) in the male urethra. The wooden portion of the pencil is radiolucent, and the lead is radiopaque.
Figure 22 demonstrates a paperclip in the male urethra.
This object is easy to identify because it is composed of metal,
and has an unusual shape.
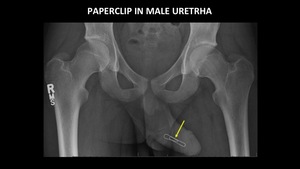
Fig. 22: AP abdominal radiograph demonstrates a paperclip (yellow arrow) in the male urethra.
PERCUTANEOUSLY INSERTED FOREIGN BODIES
Not all foreign bodies are inserted through a naturally occurring orifice.
Some patients will insert objects through intact skin or existing wounds.
Figure 23 demonstrates a straightened bed spring in the abdomen,
which is easy to identify on plain radiographs.
The patient had mental health problems and inserted this foreign body himself.
A CT was obtained due to severe abdominal pain,
which demonstrates the wire traversing a loop of bowel with adjacent fat stranding and free air.
This case demonstrates a limitation of plain radiography,
which is that small volumes of free air may not be visible.
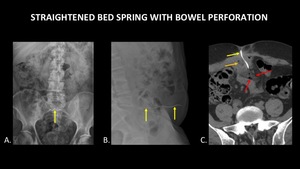
Fig. 23: AP (A) and lateral (B) radiographs demonstrate a metallic foreign body, a straightened bed spring (yellow arrows), inserted into the abdomen through the skin. Axial CT of the abdomen (C) shows this spring (yellow arrow) traversing a loop of bowel (orange arrow), with adjacent fat stranding and free air (red arrows). This case demonstrates a limitation of plain radiography, which is that serious injuries and small volumes of free air may not be apparent.
As with foreign body ingestion,
some patients will insert multiple foreign bodies.
Therefore,
it is important to obtain accurate history from the patient when possible,
and to search for additional foreign bodies once one is found.
The following examples demonstrate multiple foreign bodies inserted via different routes.
Figure 24 demonstrates a pen in the male urethra,
razorblades in the rectum and a partially imaged metallic foreign body in the right lower quadrant which was found to represent a wire in the retroperitoneum at surgery.
The patient inserted the wire through a previously existing abdominal wound.
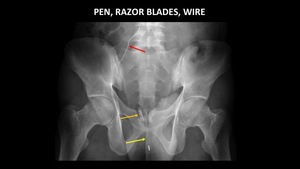
Fig. 24: AP abdominal radiograph demonstrates a pen (yellow arrow) in the male urethra and razor blades (orange arrow) in the rectum. A partially imaged thin, metallic foreign body (red arrow) in the right lower quadrant was removed at surgery, and found to represent a wire in the retroperitoneum which had been inserted through a previously existing abdominal wound.
Figure 25 demonstrates an electrical plug in the rectum,
and a wire in the male urethra.
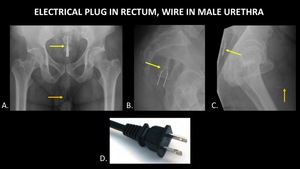
Fig. 25: AP abdominal radiograph (A) demonstrates an electrical plug (yellow arrow) in the rectum and a wire (orange arrow) in the male urethra. Sagittal radiographs of the pelvis (B, C) demonstrate the electrical plug (yellow arrow) in the rectum and wire (orange arrow) in the urethra. A photograph (D) of a similar electrical plug is included for reference.
IATROGENIC FOREIGN BODIES
Some iatrogenic foreign bodies are the result of migration or perforation of purposefully placed items.
Figure 26 demonstrates a pancreatic stent which migrated to the sigmoid colon.
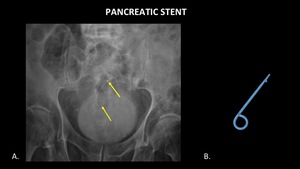
Fig. 26: AP abdominal radiograph (A) demonstrates a migrated pancreatic stent (yellow arrows) in the sigmoid colon. A photograph (B) of a pancreatic stent has been included for reference.
Figure 27 demonstrates a piece of a percutaneous gastrostomy tube which broke off and migrated through the bowel.
The item passed slowly,
but without complication.
Increased density on the surface of the object is due to mineralization,
which is consistent with the history of slow transit.
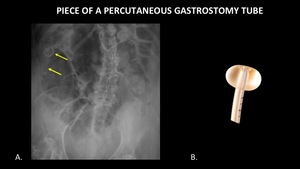
Fig. 27: AP abdominal radiograph (A) demonstrates a foreign body (yellow arrows) in the right upper quadrant consistent with a piece of a percutaneous gastrostomy tube which broke off and migrated within the bowel. A photograph (B) of the corresponding piece of a percutaneous gastrostomy tube is included for reference.
Figure 28 demonstrates two different cases of complete intrauterine device perforation and migration.
In the first case (A,
B,
C),
the device remains in the pelvis.
In the second case (D,
E),
the object migrates all the way to the right upper quadrant.
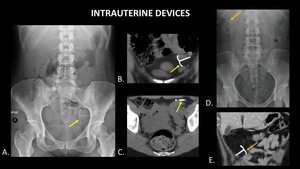
Fig. 28: AP abdominal radiograph (A), coronal CT (B) and axial CT (C) demonstrate an intraperitoneal intrauterine device (yellow arrows) in the pelvis. AP abdominal radiograph (D) and coronal CT (E) demonstrate an intraperitoneal intrauterine device (orange arrows) in the right upper quadrant of a different patient.
References: (A, B, C): Radiology, University of Massachusetts Medical School - Worcester/US. (D, E): Nowitzki KM, Hoimes ML, Chen B, Zheng LZ, Kim YH. Ultrasonography of intrauterine devices. Ultrasonography. 2015;34(3): 183-194.
One must be aware that once in the peritoneal space,
items can travel a great distance.
Capsule endoscopy is a valuable tool for evaluating the small bowel.
Before endoscopy,
patients ingest a dissolvable patency capsule with the same dimensions as the capsule endoscope to ensure the scope will pass completely through the GI tract.
This patency capsule has cellophane walls,
and is filled with barium and lactose.
If the patency capsule becomes lodged in the bowel,
it will dissolve.
However,
in very rare cases,
complications such as obstruction can occur.
Figure 29 demonstrates a patency capsule in the right lower quadrant with evidence of bowel obstruction (A).
This is a very rare complication.
The same figure also demonstrates a capsule endoscope in a different patient without evidence of complication (B).
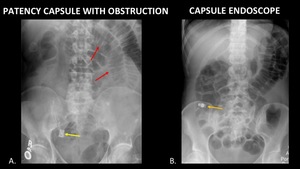
Fig. 29: AP abdominal radiograph (A) demonstrates a patency capsule (yellow arrow) in the right lower quadrant at the expected location of the terminal ileum. Dilated loops of small bowel (red arrows) are consistent with a small bowel obstruction. AP abdominal radiograph (B) demonstrates a capsule endoscope (orange arrow) in the right lower quadrant, without evidence of obstruction or other complication.
The incidence of retained surgical instruments is not well known,
but the number is estimated to be approximately 1 in 1000 abdominal surgeries.
Retained surgical instruments can result in significant morbidity and mortality.
Therefore,
it is important to make the diagnosis early.
Figure 30 demonstrates a large malleable retractor in the abdomen of a patient who presented to the emergency room with abdominal pain 2 weeks after having abdominal surgery at another institution.
Unfortunately,
no plain radiograph is available,
but the CT scout serves as a rough estimate of what the plain film would look like.
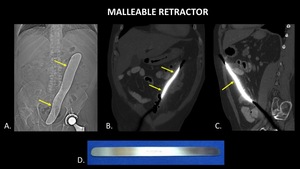
Fig. 30: Scout image (A) for abdominal CT demonstrates a large metallic foreign body (yellow arrows) projecting over the abdomen. Coronal (B) and Sagittal (C) CT of the abdomen demonstrate a large metallic foreign body (yellow arrows) within the peritoneal cavity consistent with a malleable retractor. A photograph (D) of a malleable retractor is included for reference.
Figure 31 demonstrates a radiopaque foreign body in the right lower quadrant on a CT scout image.
Unfortunately,
no plain radiograph is available.
CT images demonstrate the same radiopaque foreign body in the right lower quadrant,
within an encapsulated mass.
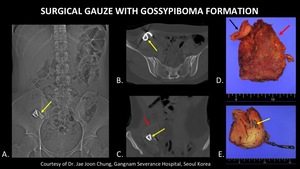
Fig. 31: Scout image (A) from abdominal CT demonstrates a radiopaque foreign body (yellow arrow) in the right lower quadrant. Axial (B) and Coronal (C) CT images demonstrate the same radiopaque foreign body (yellow arrows) in the right lower quadrant, within an encapsulated mass (red arrow). Photograph (D) of the gross specimen after the object was surgically removed demonstrates a piece of surgical gauze (black arrow) within an encapsulated mass (red arrow), corresponding to the foreign body and encapsulated mass seen on CT. Photograph (E) of the cut specimen demonstrates a mass of surgical gauze containing blue components (yellow arrows) corresponding to the radiopaque marker seen on the scout and CT.
References: Courtesy of Dr. Jae Joon Chung, Gangnam Severance Hospital, Seoul/Korea
The foreign body was surgically removed,
and found to represent a piece of retained surgical gauze from recent cesarean section surrounded by a mass of granulation tissue. This is known as a Gossypiboma.
It is important to recognize retained surgical gauze early because serious complications,
including death,
can occur.
To understand how retained surgical instrument events occur,
one must think about the typical surgical suite.
Figure 32 demonstrates a typical operating room table (A) with multiple surgical instruments,
and a gauze counting rack (B).
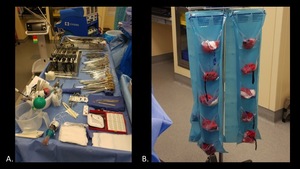
Fig. 32: Photographs demonstrate a typical operating room table (A) with multiple surgical instruments, and a gauze counting rack (B).
Although there is an instrument count after every surgery,
human error is still possible.
Gauze is one of the most common retained foreign bodies after surgery.
Therefore,
it is essential for radiologists to be familiar with the appearance of surgical gauze on radiographs.
All surgical gauze is impregnated with radiopaque material to aid in detection.
This is because the gauze itself is relatively radiolucent.
Figure 33 demonstrates the appearance of surgical gauze on radiographs.
Please be aware that not all gauze has the same appearance.
Gauze comes in many shapes and sizes,
and the markers are varied as well.
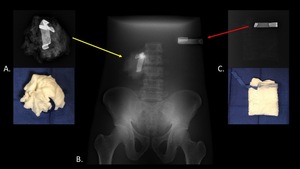
Fig. 33: Radiographs and photographs of wet, balled up (A) and dry, folded (C) surgical gauze were obtained to demonstrate the varied radiographic appearance of surgical gauze. Note that the wet gauze is more radiopaque than the dry gauze, but both can be identified by the very radiopaque marker. Both pieces of gauze were radiographed behind a phantom (B) to approximate the appearance in a patient.
Figure 34 demonstrates the appearance of peanut dissector gauze.
The radiograph demonstrates the importance of the radiopaque strings for identifying these tiny objects on post-operative x-rays.
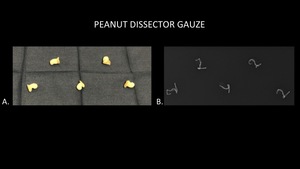
Fig. 34: Photograph (A) and radiograph (B) of peanut dissector gauze. The radiograph demonstrates the importance of the radiopaque strings for identifying these tiny objects on post-operative x-rays.
In some cases,
one may not know what the foreign body of interest looks like on x-ray.
If available,
it may be helpful to place a similar reference object next to the patient when the x-ray is taken (Figure 35).

Fig. 35: AP abdominal radiograph of the abdomen demonstrates a metallic ring (yellow arrow) in the stomach of a child, and a similar ring (orange arrow) placed at the patient’s side for reference.
Knowing what you are looking for will increase your chances of finding the object of interest.


 demonstrate foreign bodies composed of metal, including batteries (yellow arrow), nails (orange arrows), and a screw (red arrow).")
 (yellow arrows) is almost completely radiolucent, and is identified by the presence of straight lines in the body and air within the tube. A pen and toothbrush (B) inserted next to one another are more easily identified due to the presence of radiopaque components, such as the tip of the pen (orange arrow) and tongue scraper on the toothbrush (red arrow). The plastic components are radiolucent (yellow arrows).")
 and plant-based material (B). Both foreign bodies are indicated with yellow arrows.")
 though the GI tract, from the stomach (A), to the small bowel (B), and large bowel (C).")
 in the stomach.")
, coronal abdominal CT (B), and sagittal abdominal CT (C) demonstrate fragments of a broken pencil within the stomach (yellow arrows). Radiopaque lead (orange arrows) within the pencil fragments aids in foreign body detection on both plain radiograph and CT. The wooden portion of the pencil is radiolucent, with a density similar to air.")
 demonstrates multiple round magnets (yellow arrows) within the stomach of a child. A photograph (B) of a block made of this type of magnet is provided for reference.")
 demonstrates two thin, curvilinear densities in the right upper quadrant (yellow arrows), one of which projects over cholecystectomy clips. Coronal abdominal CT (B) demonstrates a thin, metallic foreign body (yellow arrow) perforating through the gastric antrum. Axial abdominal CT (C) demonstrates a thin, metallic foreign body (yellow arrow) within the peritoneal cavity, abutting the liver. In this case, there is no free air or fat stranding, and the patient did not demonstrate signs of peritonitis.")
 in the large bowel. Note the uniform shape, size and density of the objects.")
, including a pen (A), springs (B), a razor blade (C), and open safety pin (D).")
 demonstrates a toothbrush and pen (yellow arrows) in the rectosigmoid colon. These objects are almost entirely radiolucent, but radiopaque components including the tongue scraper on the toothbrush (red arrow) and tip of the pen (orange arrow) aid in detection. Photographs (B, C) of a similar toothbrush and pen refill are included for reference.")
 demonstrates a plastic travel toothbrush case (yellow arrows) in the rectum. The object is relatively radiolucent, but more easily detected due to its straight contours and the air it contains. A photograph (B) of a similar toothbrush case is provided for reference.")
 demonstrates an aerosol can (yellow arrows) in the rectum. A photograph (B) of a similar can is included for reference.")
 in the rectum.")
 and Sagittal radiograph (B) of the pelvis demonstrate a silicone object (yellow arrows) in the form of male genitalia in the rectum.")
 and sagittal abdominal CT (B) demonstrate a cucumber (yellow arrows) in the rectosigmoid colon. A photograph (C) of a cucumber is included for reference.")
 demonstrates a wooden rolling pin (yellow arrows) in the rectosigmoid colon. This was complicated by bowel perforation, as evinced by free air under the diaphragm (red arrow). A photograph (B) of a similar rolling pin is included for reference.")
 demonstrate a light bulb (yellow arrow) in the rectum, and air (orange arrows) in the retroperitoneum surrounding the kidneys. Axial CT (C, D) again demonstrates the light bulb in the rectum (yellow arrow) and confirms pneumoretroperitoneum (orange arrows).")
 demonstrates a small shampoo bottle (yellow arrows) in the rectum. Axial abdominal CT (B) demonstrates the bottle (yellow arrow) in the rectum, abutting an enlarged, edematous left seminal vesicle (red arrow). Trace free fluid was also present in the pelvis (not pictured). Findings are consistent with left seminal vesicle injury due to trauma from foreign body insertion. Sagittal abdominal CT (C) demonstrates the partially filled bottle (yellow) in the rectum, with an air fluid level in the bottle. A photograph (D) of a similar type of bottle is included for reference.")
 in the vagina.")
 in the male urethra. The wooden portion of the pencil is radiolucent, and the lead is radiopaque.")
 in the male urethra.")
 and lateral (B) radiographs demonstrate a metallic foreign body, a straightened bed spring (yellow arrows), inserted into the abdomen through the skin. Axial CT of the abdomen (C) shows this spring (yellow arrow) traversing a loop of bowel (orange arrow), with adjacent fat stranding and free air (red arrows). This case demonstrates a limitation of plain radiography, which is that serious injuries and small volumes of free air may not be apparent.")
 in the male urethra and razor blades (orange arrow) in the rectum. A partially imaged thin, metallic foreign body (red arrow) in the right lower quadrant was removed at surgery, and found to represent a wire in the retroperitoneum which had been inserted through a previously existing abdominal wound.")
 demonstrates an electrical plug (yellow arrow) in the rectum and a wire (orange arrow) in the male urethra. Sagittal radiographs of the pelvis (B, C) demonstrate the electrical plug (yellow arrow) in the rectum and wire (orange arrow) in the urethra. A photograph (D) of a similar electrical plug is included for reference.")
 demonstrates a migrated pancreatic stent (yellow arrows) in the sigmoid colon. A photograph (B) of a pancreatic stent has been included for reference.")
 demonstrates a foreign body (yellow arrows) in the right upper quadrant consistent with a piece of a percutaneous gastrostomy tube which broke off and migrated within the bowel. A photograph (B) of the corresponding piece of a percutaneous gastrostomy tube is included for reference.")
, coronal CT (B) and axial CT (C) demonstrate an intraperitoneal intrauterine device (yellow arrows) in the pelvis. AP abdominal radiograph (D) and coronal CT (E) demonstrate an intraperitoneal intrauterine device (orange arrows) in the right upper quadrant of a different patient. References: (A, B, C): Radiology, University of Massachusetts Medical School - Worcester/US. (D, E): Nowitzki KM, Hoimes ML, Chen B, Zheng LZ, Kim YH. Ultrasonography of intrauterine devices. Ultrasonography. 2015;34(3): 183-194.")
 demonstrates a patency capsule (yellow arrow) in the right lower quadrant at the expected location of the terminal ileum. Dilated loops of small bowel (red arrows) are consistent with a small bowel obstruction. AP abdominal radiograph (B) demonstrates a capsule endoscope (orange arrow) in the right lower quadrant, without evidence of obstruction or other complication.")
 for abdominal CT demonstrates a large metallic foreign body (yellow arrows) projecting over the abdomen. Coronal (B) and Sagittal (C) CT of the abdomen demonstrate a large metallic foreign body (yellow arrows) within the peritoneal cavity consistent with a malleable retractor. A photograph (D) of a malleable retractor is included for reference.")
 from abdominal CT demonstrates a radiopaque foreign body (yellow arrow) in the right lower quadrant. Axial (B) and Coronal (C) CT images demonstrate the same radiopaque foreign body (yellow arrows) in the right lower quadrant, within an encapsulated mass (red arrow). Photograph (D) of the gross specimen after the object was surgically removed demonstrates a piece of surgical gauze (black arrow) within an encapsulated mass (red arrow), corresponding to the foreign body and encapsulated mass seen on CT. Photograph (E) of the cut specimen demonstrates a mass of surgical gauze containing blue components (yellow arrows) corresponding to the radiopaque marker seen on the scout and CT. References: Courtesy of Dr. Jae Joon Chung, Gangnam Severance Hospital, Seoul/Korea")
 with multiple surgical instruments, and a gauze counting rack (B).")
 and dry, folded (C) surgical gauze were obtained to demonstrate the varied radiographic appearance of surgical gauze. Note that the wet gauze is more radiopaque than the dry gauze, but both can be identified by the very radiopaque marker. Both pieces of gauze were radiographed behind a phantom (B) to approximate the appearance in a patient.")
 and radiograph (B) of peanut dissector gauze. The radiograph demonstrates the importance of the radiopaque strings for identifying these tiny objects on post-operative x-rays.")
 in the stomach of a child, and a similar ring (orange arrow) placed at the patient’s side for reference.")