The pancreaticoduodenal groove (PDG) is a small theoretic space defined :
Medially by the pancreatic head,
Laterally by the second portion of the duodenum (D),
Posteriorly by the third portion of the duodenum (D) and inferior vena cava,
Superiorly by the duodenal bulb.
The distal common bile duct (CBD),
main pancreatic duct (MPD),
accessory pancreatic duct,
major papilla,
and minor papilla (MP) are found in the pancreaticoduodenal groove.
A number of small arteries and veins lie within this space,
the most important of which is the superior pancreaticoduodenal artery [1].
Groove pancreatitis (GP) is a rare form of chronic pancreatitis,
which has to be distinguished from pancreatic adenocarcinoma. Two forms of groove pancreatitis have been described: the pure form,
which affects only the groove,
and the segmental form,
which involves the pancreatic head with development of scar tissue within the groove [2].

Fig. 1: Pictorial illustration of paraduodenal pancreatitis(PP)depicting a fibroinflammatory mass in the pancreatico-duodenal groove (PDG) with concurrent duodenal and paraduodenal cysts (C) in the region of minor papilla (MP). P: Pancreas; DS: Duct of Santorini; DW: Duct of Wirsung
References: Arora A et al. (2015) Clinicoradiological appraisal of 'paraduodenal pancreatitis': Pancreatitis outside the pancreas! Indian J Radiol Imaging 2015;25:303-14
While the pathogenesis of groove pancreatitis is still unclear,
several mechanisms have been proposed: functional obstruction of the minor papilla or duct of Santorini,
increasingly viscous pancreatic juice as a result of alcohol use and smoking,
Brunner gland hyperplasia resulting in stasis of pancreatic secretions,
heterotopic pancreas in the duodenum and peptic ulcer disease [3].
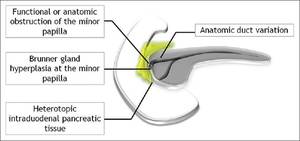
Fig. 2: Etiopathogenesis of paraduodenal pancreatitis
References: Arora A et al. (2015) Clinicoradiological appraisal of 'paraduodenal pancreatitis': Pancreatitis outside the pancreas! Indian J Radiol Imaging 2015;25:303-14
Alcohol consumption seems to be the strongest association.
Therefore,
patients with groove pancreatitis are typically middle-aged men with a history of significant alcohol abuse.
The clinical presentation depends on the acuity.
Some patients in the acute setting present with severe abdominal pain,
nausea,
vomiting,
or even acute gastric outlet obstruction,
whereas patients with chronic presentation often have evidence of jaundice or chronic weight loss,
signs more frequently indicative of malignancy [3,4].
Biochemical markers are of limited use for the distinction between groove pancreatitis and pancreatic adenocarcinoma.
Pancreatic enzymes are usually normal or only minimally elevated.
Bilirubin levels can be elevated in the presence of CBD obstruction,
while alkaline phosphatase levels can be elevated even in the absence of ductal obstruction. Tumor markers (e.g.
carcinoembryonic antigen and CA-19-9) are usually negative [3,5].
Histopathologically,
a variable degree of thickening and scarring of the duodenal wall in the vicinity of minor papilla is observed [6].
The scarring process involves the distal CBD,
the groove and the adjacent pancreatic head in the segmental form.
Cystic changes may be found in the duodenal wall or in the groove.
The cysts can reach large size and fluctuate depending on the activity of the disease.
They represent dilated accessory duct of Santorini and its branches and may indent or compress the CBD.
The duodenum is almost always involved.
Brunner’s gland hyperplasia is typically prominent and is largely responsible for the thickening of the duodenal wall [3].
Heterotopic pancreatic tissue is also visualized in some cases and is considered a predisposing factor for groove pancreatitis [4].
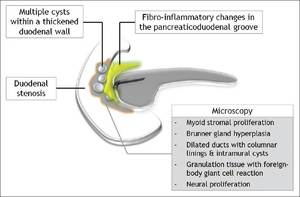
Fig. 3: Schematic illustration of the pathological manifestations of paraduodenal pancreatitis
References: Arora A et al. (2015) Clinicoradiological appraisal of 'paraduodenal pancreatitis': Pancreatitis outside the pancreas! Indian J Radiol Imaging 2015;25:303-14
Adsay et al.
introduced the term ”paraduodenal pancreatitis” to include pathologic entities with common characteristics (myoid stromal proliferation,
Brunner gland hyperplasia,
granulation tissue with foreign-body giant reaction,
fibrosis,
dilated ducts and intramural cysts),
like ”cystic dystrophy of heterotopic pancreas”,
“paraduodenal wall cysts”,
and “groove pancreatitis”[6].
Groove pancreatitis may be treated conservatively with analgesics,
pancreatic rest and abstinence from alcohol,
while surgery is reserved for cases of untreatable pain or to rule out malignancy in equivocal cases [3].

depicting a fibroinflammatory mass in the pancreatico-duodenal groove (PDG) with concurrent duodenal and paraduodenal cysts (C) in the region of minor papilla (MP). P: Pancreas; DS: Duct of Santorini; DW: Duct of Wirsung References: Arora A et al. (2015) Clinicoradiological appraisal of 'paraduodenal pancreatitis': Pancreatitis outside the pancreas! Indian J Radiol Imaging 2015;25:303-14")
 Clinicoradiological appraisal of 'paraduodenal pancreatitis': Pancreatitis outside the pancreas! Indian J Radiol Imaging 2015;25:303-14")
 Clinicoradiological appraisal of 'paraduodenal pancreatitis': Pancreatitis outside the pancreas! Indian J Radiol Imaging 2015;25:303-14")