ECR 2018 / C-2167
Prostate gland multiparametric resonance. From guidelines to practice.
Congress:
ECR 2018
Poster Number:
C-2167
Type:
Educational Exhibit
Keywords:
MR, Oncology, MR-Functional imaging, Diagnostic procedure, Education, Cancer, Education and training
Authors:
C. Gómez 1, L. A. Ruiz Elizondo2; 1México /MX, 2Mexico City/MX
DOI:
10.1594/ecr2018/C-2167

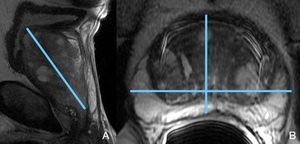
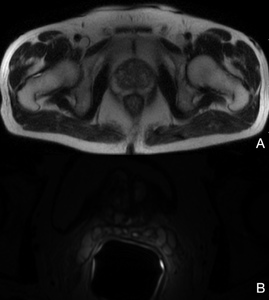
Fig. 14:
T2WI A. Sagittal midline. B. axial towards the base.

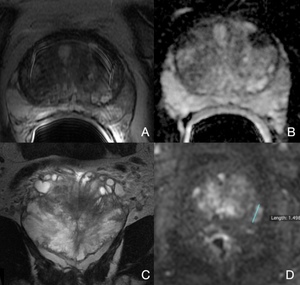
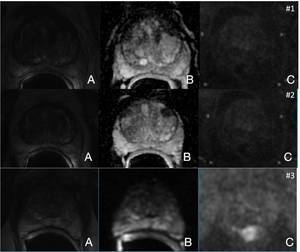
Fig. 16:
Patient 1 TZ evaluation, lesion #2, Gland base A. axial T2WI B. ADC C. DCE D....

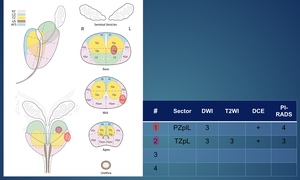
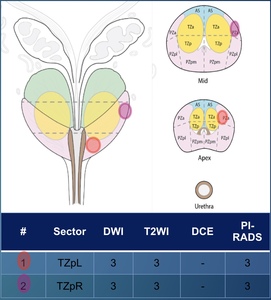
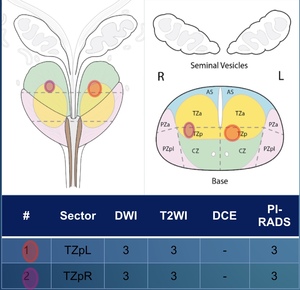
Fig. 17:
Patient 1 Sector map and lesion index.

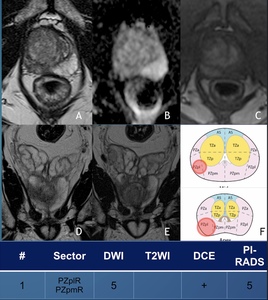
Fig. 18:
Patient 1 additional findings A. axial T2WI with broad FoV for pelvic...

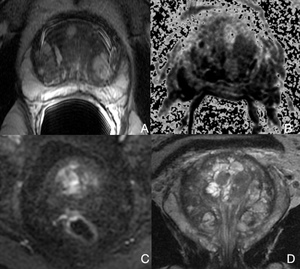
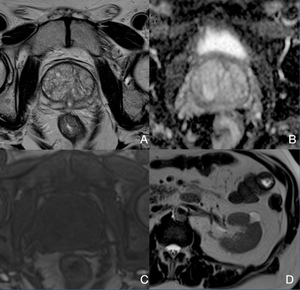
Fig. 19:
Patient 2 Prostatic base. A. T2WI B. ADC C. DCE D. Axial T2WI upper abdomen.

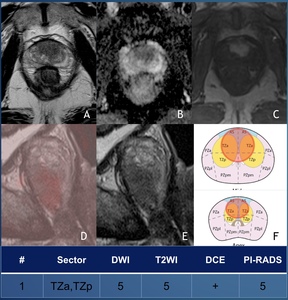
Fig. 20:
Patient 3 A. T2WI B. ADC C.DCE D. Fused T2W/DCE E. sagittal T2WI F. Sector map....

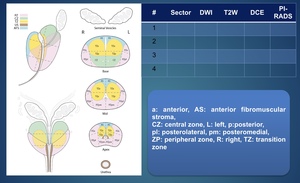
Fig. 24:
Sector map.

Fig. 26:
Patient 5 Sector map

Fig. 27:
Patient 6. A. T2WI B. ADC C.DCE D. And E. Coronal T2WI, F. Sector map.

Fig. 21:
Patient 4 Lesion #1 prostatic apex. A. T2WI B. ADC C. DCE

Fig. 23:
Axial T2WI, demonstrating bilateral renal cysts. B. Axial T2WI, pancreatic tail...

Fig. 22:
Patient 4 Lesion #2 Mid portion. A. T2WI B. ADC C. DCE.

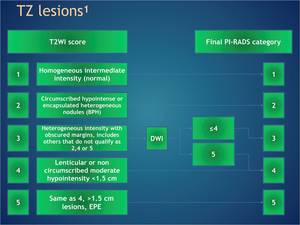
Table 3:
TZ lesions reading algorithm.