In the approach of unilateral hemithorax hyperlucency,
technical and positional factors have to be excluded first,
and then pathology may be considered,
thinking that the decrease in pulmonary density may be the result from a combination of changes in the relative amounts of air,
blood,
and interstitial tissue,
and by changes on any of the anatomic structures traversed by the x-rays.
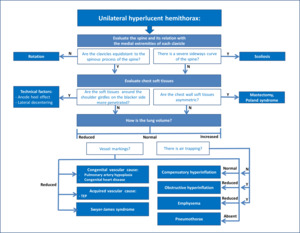
Fig. 32: In the approach of unilateral hyperlucent hemithorax, technical factors and chest wall abnormalities are the possible causes to be considered first.
By checking the spine and its relation with the medial ends of each clavicle, in addition to the position of mediastinum, one can easily rule out the existence of scoliosis or patient rotation.
Then by checking the relative exposure of soft tissues in the affected side (especially around the shoulder girdles) one may infer if faulty radiologic technique is at stake producing a false-positive. Any asymmetry on chest wall soft tissues should also be noted as this could be the cause of the differential transradiancy.
When evaluating the lung area one must may pay special attention to lung volume and its vascular markings, as hyperexpansion, with or without air trapping, and alteration in vasculature, are the most important mechanisms in the pathophysiology of a hyperlucent lung.
Any clinical evidence of central airway, pulmonary vascular and lung parenchymal abnormality should be considered when formulating differential diagnosis, and one should also consider the age of the patient as well as previously existing neoplastic or infectious disease, as these may also provide important diagnostic information.
It may also be usefull to use a mnemonic for easy memorizing of unilateral hypertranslucent hemithorax differential diagnosis, e.g.:
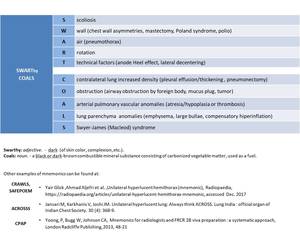
Fig. 33: Mnemonic idealized for unilateral hyperlucent hemithorax differential diagnosis.
