Neuroblastoma is an embrionary tumor and constitutes the second most common solid malignancy in children,
after CNS tumors,
and the third most common pediatric cancer.
It affects boys and girls in the same proportion,
with a median age at diagnosis is 16 months,
being 95% of cases diagnosed by 7 years of age.
Despite recent advances and different therapeutic options that include chemotherapy and stem cell trasplant,
it still represents 15% of cancer deaths in children.
Neuroblastoma derives from the primordial neural crest cells that form the sympathetic nervous system,
as ganglioneuroma and ganglineuroblastoma,
and constitutes the group of small round blue cells of childhood,
together with rhabdomyosarcoma,
Ewing sarcoma and lymphoma .
The precursor cells that lead to these primordial cell crest tumors may remain undifferenciated (neuroblasts) or mature (Schwann cells),
ranging from neuroblastomas if the primary cells that compose them are undifferenciated to ganglioneuromas if the predominant cells are mature.
These cells and the respective tumors derived from them may become more mature or regress,
changing from immature to more mature forms and viceversa.
This variable behaviour is also patent in the biologic features of neuroblastoma,
with some tumors that may have a relatively benign course to others potentially letal (Fig.2).
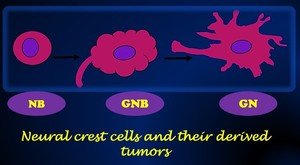
Fig. 2: Illustration of the neural crest cells tumors depending on their maturation state. (NB: Neuroblastoma, GNB: Ganglioneuroblastoma, GN: Ganglioneuroma).
The clinical presentation of neuroblastoma depends on:
1.The anatomical location of the primary tumor. As neuroblastoma derives from primordial neural crest cells that lead to the sympathetic differentiation,
they may arise anywhere sympathetic tissue naturally occurs.
The most common site for primary NBL is the adrenal medulla (35-40%),
followed by the retroperitoneum (30-35%),
the thorax (mediastinum) (20%),
the cervical region (2%) and finally the pelvis (1%).
Abdominal neuroblastomas tend to present with abdominal distension or pain caused by local effects from the primary tumor; Thoracic (mediastinal) and cervical neuroblastomas are more usually incidentally found on chest x-rays even though they can also present as a Horner syndrome (ptosis,
pupillary constriction and ipsilateral facial anhidrosis).
2.The anatomical location of metastasis.
The most common site of metastasis of neuroblastoma are the bone marrow,
followed by the skeleton,
locoregional linfadenopathies and the liver.
Bone marrow infiltration may lead to signs of haematopoietic failure,
whereas metastasis to the skeleton may lead to pain or pathological fractures in the affected bones.
A common sign of neuroblastoma are the periorbital ecchymosis or so called âracoon eyesâ,
which are due to infiltration of the bony orbit by the tumor.
In these cases,
differential diagnosis with child abuse has to be done.
3.Paraneoplastic phenomena. Neuroblastoma is a tumor that secretes cathecolamines.
Due to the effects of this hormones,
patients may present with intermittent hypertension or diarrhoea.
Other paraneoplastic phenoma present in up to 2% of the patients with neuroblastomas is the opsoclonus-myoclonus syndrome,
which consists of jerking movements of the extremities and eyes,
sometimes with verebellar ataxia.
The cause of this syndrome remains unknown nowadays.
Prognostic factors
The enigmatic nature and course of this tumor has long been recognized,
with some tumors undergoing spontaneous involution without any theraphy and others progressing with a fatal outcome.
As a consequence,
the main management strategies nowadays try to focus on wether these patients have a favorable or unfavorable disease.
For this,
there are strong prognostic factors that can accurately predict wether children have a âgoodâ or âbadâ disease at diagnosis.
These prognostic factors are:
1.
The age.
Children with more than 5 years old have worse prognosis.
2.
The serum lactate dehydrogenasa (LDH) level.
Higher LDH levels are associated with worse outcome.
3.
Presence of genetic alterations (such as n-myc alteration,
present in 30% of patients).
4.
Histologic category and grade of tumor differentiation.
5. Presurgical stage.
As complete resection of the tumor is the main prognostic factor,
accurate presurgical staging becomes essential,
which means that the radiologistsÂī role turns crutial.

.")