ECR 2018 / C-2428
Idiopathic Retroperitoneal Fibrosis: Imaging findings and differential diagnosis
Congress:
ECR 2018
Poster Number:
C-2428
Type:
Educational Exhibit
Keywords:
Aneurysms, Education, Diagnostic procedure, CT-Angiography, Ultrasound, CT, Arteries / Aorta, Abdomen, Inflammation, Haematologic diseases, Retroperitoneum
Authors:
M. Cruz, C. Ferreira, P. G. Oliveira, E. Pinto, F. Caseiro Alves; Coimbra/PT
DOI:
10.1594/ecr2018/C-2428
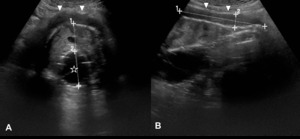
 in a patient with an aortic aneurysm submitted to an endovascular aneurysm repair (star). Note that it presents as a homogeneously hypoechoic band enfolding the aorta on axial [A] and longitudinal [B] planes. This finding was initially interpreted as an endoleak.")
Fig. 1:
Idiopathic Retroperitoneal Fibrosis on ultrasound (arrowheads) in a patient...

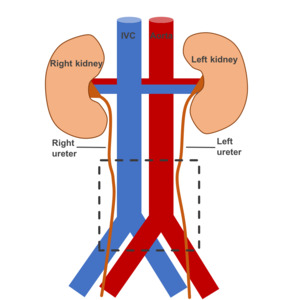
Fig. 2:
Typical location of Idiopathic Retroperitoneal Fibrosis, represented by the...
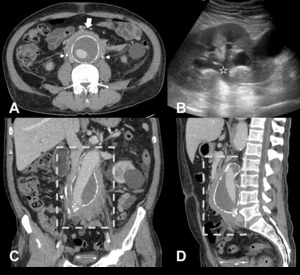
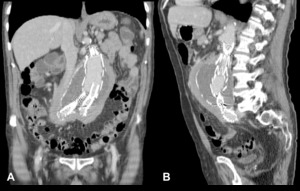
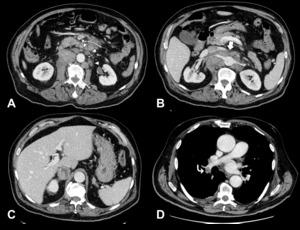
 wraps the infrarenal aorta while sparing the posterior border. Two ureteral stents are depicted (arrowheads). [B] – Ultrasound shows hydronephrosis (star) secondary to ureteral obstruction. [C] and [D] – Coronal and sagittal reformations show the typical extent of Idiopathic RPF (dashed rectangle).")
Fig. 3:
Idiopathic retroperitoneal fibrosis causing bilateral ureteral obstruction in a...
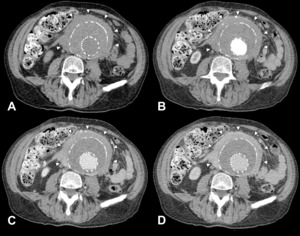
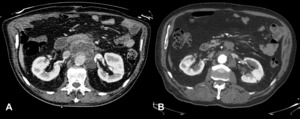
. The mass wrapping the infra-renal aorta (arrowheads) has spontaneous attenuation similar to the paraspinal muscles [A]. The dynamic study in the arterial [B], portal [C] and late [D] phases demonstrated a mild, homogeneous and progressive enhancement.")
Fig. 4:
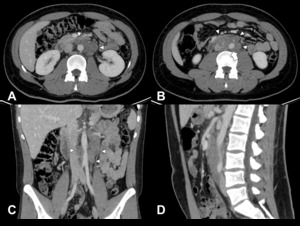
Idiopathic Retroperitoneal Fibrosis on CT (same case illustrated in Fig. 1)....

Fig. 5:
Coronal [A] and sagittal [B] CT reformations of the case illustrated in Fig. 4....
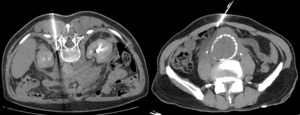
 collected along the anterior and left lateral borders of the aorta in a 75 year-old male patient. [B] – Secondary Retroperitoneal Fibrosis (arrowheads) was depicted in the same location on follow-up examination (one year later, after antibiotherapy and percutaneous drainage of the collections).")
Fig. 6:
[A] – Contrast-enhanced CT revealed an infected aortic graft leak with...

Fig. 7:
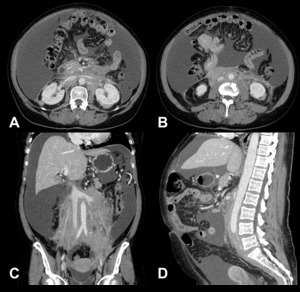
Secondary Retroperitoneal Fibrosis due to Erdheim-Chester disease in a...
. Note the involvement at the level of the renal hila [A], the floating aorta sign [B, arrow] and the extent of the disease on coronal [C] and sagittal [D] reformations. Massive ascites is evident.")
Fig. 8:
Secondary Retroperitoneal fibrosis in a 59-year-old female patient due to a...

Fig. 9:
Secondary Retroperitoneal fibrosis due to a Diffuse Large B-Cell Lymphoma. From...

Fig. 10:
Secondary Retroperitoneal Fibrosis in a 21 year-old male patient due to a...
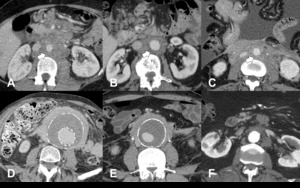
 is represented in the top three cases, which have a malignant ethiology [A-C]. Compare them with the benign cases from the bottom row [D-F] where this sign is absent.
[A and B] – Lymphomas. [C] – Metastatic carcinoma of unknown origin (same case as in Fig. 8). [D and E] – Idiopathic RPF (same cases as in Figs. 3 and 4). [F] – Secundary RPF due to an infected aortic graft leak (same case as in Fig. 6).")
Fig. 11:
The floating aorta sign (arrows) is represented in the top three cases, which...
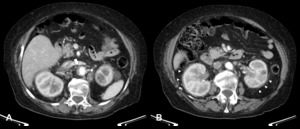
. B – Histopathological study confirmed retroperitoneal fibrosis without neoplastic cells (same patient as in Fig. 3).")
Fig. 12:
CT-guided biopsy of two retroperitoneal masses. A – Histopathological study...