ECR 2018 / C-2439
Bone Marrow Edema in the Knee: A pictorial Review
Congress:
ECR 2018
Poster Number:
C-2439
Type:
Educational Exhibit
Keywords:
Metabolic disorders, Inflammation, Diagnostic procedure, MR, Musculoskeletal system, Musculoskeletal joint, Musculoskeletal bone
Authors:
J. Saraiva1, A. S. Teixeira Gomes2, C. Bilreiro1, A. R. Ventosa1, R. Monteiro1, B. M. Q. Santos1, M. O. E. Castro1; 1Portimao/PT, 2Lisbon/PT
DOI:
10.1594/ecr2018/C-2439
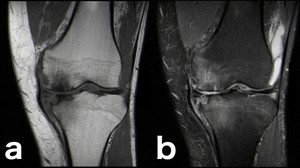
: 58-year-old man with extensive chondral defect at the weight-bearing area of the medial femoral condyle, associated with small marginal osteophytes and secondary subchondral bone marrow edema. Osteoarthritis isn’t usually classified alongside traumatic etiologies but rather as a degenerative condition, truth is that the development of BME on OA is secondary to repetitive microtrauma on weight-bearing structures[2] (a: coronal T1-WI; b: coronal PD-FS-WI; c: sagittal PD-FS-WI).")
Fig. 2:
Osteoarthritis (OA): 58-year-old man with extensive chondral defect at the...
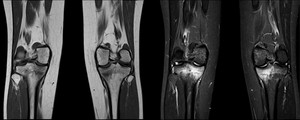
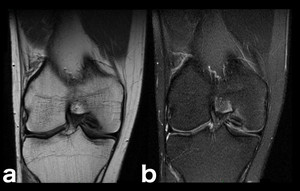
 fractures: T1-weighted and STIR coronal images of the knees of a 25-year-old woman, who had recently engaged in strenuous physical activity at the gym without adequate conditioning. She complained of medial tibial pain bilaterally. Medial proximal stress fractures are evident in both tibias.")
Fig. 3:
Stress (fatigue) fractures: T1-weighted and STIR coronal images of the knees of...
 and on T2-FS-WI (c). On the water-sensitive sequence (T2-FS-WI) the hyperintense bone marrow edema surrounding the fracture is evident, while on the T1-WI’s it translates as an ill-defined hypointense area on the otherwise hyperintense marrow of the distal femoral epiphysis and proximal tibia.")
Fig. 7:
Trabecular microfracture: 15-year-old male adolescent with acute pain following...
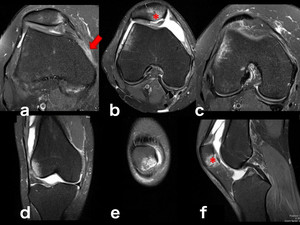
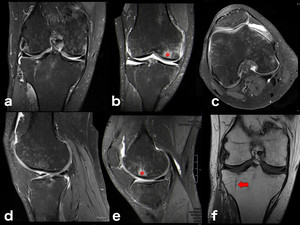
, coronal (d, e) and sagittal planes (f) of a young adult with transient patellar dislocation and resulting typical contusion pattern: anterolateral aspect of the lateral femoral condyle and inferomedial aspect of the patella. It’s more common on teenagers or young adults who perform sports that require a twisting motion of the knee while it’s flexed. Associated lesions can be present, as in this patient with osteochondral injury of the patella (*) and tear of the medial patellofemoral ligament (MPFL) (arrow).")
Fig. 8:
Traumatic bone edema, patellar dislocation typical pattern: PD-FS-WI on axial...
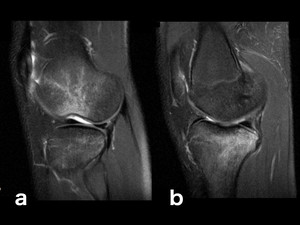
.[3] The degree of flexion of the knee determines the exact location of the lateral femoral condyle injury (more flexion results in a more posterior bruise, whereas less flexion results in a more anteriorly located edema).[3] Sometimes, as shown in a, a lateral femoral condyle impaction fracture occurs. Another frequently associated site of bone contusion is the posterior aspect of the medial tibial plateau (as shown in b), thought to result from contrecoup forces in the medial compartment at the resolution of the forced valgus forces (b). The ACL is frequently disrupted in this kind of trauma[3], therefore when this pattern is recognized a thorough evaluation of the ligament should be performed.")
Fig. 9:
Traumatic bone edema, typical pivot shift pattern: PD-FS-WI on sagittal planes....
.")
Fig. 10:
Traumatic bone edema, typical pivot shift pattern: T2-FS-WI on sagittal planes,...

Fig. 11:
Traumatic bone edema, typical clip injury pattern: Trauma sustained by a...
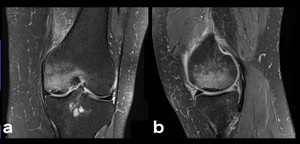
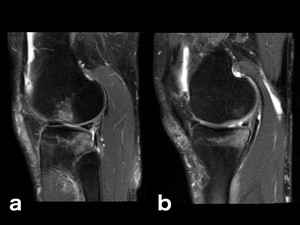
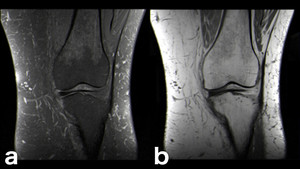
. Now it’s considered to be an insufficiency fracture.[5] These insufficiency fractures typically develop at the medial femoral condyle and in the femoral head and are present in older individuals (they are related to osteoporosis and altered biomechanics, as in unstable meniscal lesions).[5] Similar to other stress fractures, a hypointense fracture line is surrounded by hyperintense bone marrow edema on water-sensitive sequences (a, b: coronal and sagittal PD-FS-WI).")
Fig. 4:
SIF: in the past, every time a subchondral lesion as this one was observed in...
.")
Fig. 5:
Long-standing SIF with subchondral collapse and associated large area of edema...
.")
Fig. 6:
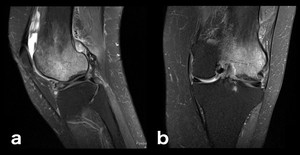
Less common form of SIF on the medial tibial plateau (a, b: sagittal and...
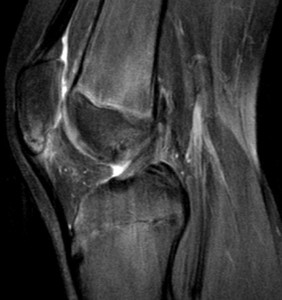
: This patient had a very faint fracture line on conventional radiography, barely noticeable (not shown here). On MR imaging the contusional bone edema surrounding the fracture makes it impossible to miss (PD-FS-WI hyperintensity and T1-WI hypointensity on the lateral tibial plateau). The fracture line is hypointense on T1-WI (a, c) and isointense on PD-FS-WI (b, d).")
Fig. 12:
Traumatic bone edema, macroscopic fracture (with cortical disruption): This...
: When the posterior cruciate ligament is not retracted it can be hard to identify an avulsion fracture of its insertion. The surrounding bone edema makes it an easier diagnosis.")
Fig. 13:
Traumatic bone edema, macroscopic fracture (PCL avulsion): When the posterior...
, MRI bone edema points out where to look (c, d, e, f).")
Fig. 14:
Traumatic bone edema, macroscopic subacute fracture: Even with a little less...
 in both the unfused accessory ossification center and the remaining patella (a, b: coronal and axial PD-FS-WI).")
Fig. 15:
Up to 2% of all bipartite patellae become painful because of stress across the...
.")
Fig. 16:
Osgood-Schlatter’s disease is a chronic avulsion injury thought to result...
.")
Fig. 17:
This 13-year-old boy has Sinding-Larsen-Johansson Syndrome, a chronic traction...
. OCD etiology is unknown and likely multifactorial, with injury, vascular factors, pressure changes, developmental differences, and genetics all contributing.[5] The most common site for OCD of the knee is the lateral aspect of the medial femoral condyle (75%).[5] Here is shown a characteristic MRI appearance, typically without additional lesions: a small area of bone marrow edema is evident on b, surrounding the osteochondral fragment. (a, b: coronal T1-WI and coronal PD-FS-WI).")
Fig. 18:
Osteochondritis dissecans (OCD). OCD etiology is unknown and likely...
. Same patient as in fig. 18. An osteochondral fragment on the lateral aspect of the right femoral medial condyle is seen on conventional radiography.")
Fig. 19:
Osteochondritis dissecans (OCD). Same patient as in fig. 18. An osteochondral...
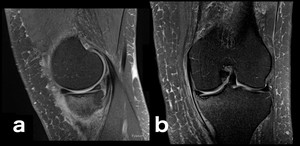
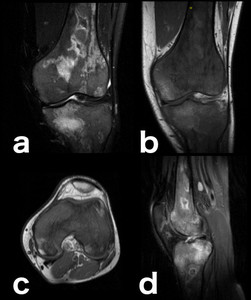
 are prone to develop osteonecrosis secondary to capillary obstruction. This obstruction leads to raised capillary hydrostatic pressure, which in turn is responsible for the hyperintense edema surrounding the hypointense bone infarcts on water-sensitive sequences. This is an example of BME of a congestive nature (due to impaired removal of fluid from the marrow space capillary bed). This patient also presents extensive red marrow reconversion as depicted on the marrow signal in T1-WI’s (much lower than surrounding fat tissue and slightly higher than muscle tissue) and DP-FS-WI’s (doesn’t fully saturate, remaining slightly hyperintense) (a: coronal DP-FS-WI; b: coronal T1-WI; c: axial T1-WI; d: sagittal DP-FS-WI).")
Fig. 20:
Patients with hemoglobinopathies (for instance sickle-cell anemia, as in this...
 (a, b: coronal T1-WI and PD-FS-WI).")
Fig. 21:
This patient’s inflammatory arthritis is responsible for the bone marrow...
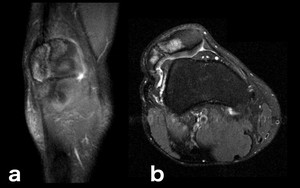
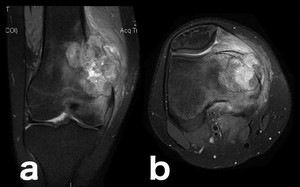
: tumorigenic edema is secondary to direct capillary trauma from trabecular destruction with the release of intravascular fluid and associated hemorrhage.[2] It may be difficult to differentiate surrounding edema from tumor invasion.")
Fig. 22:
Osteosarcoma (a, b: coronal and axial PD-FS-WI): tumorigenic edema is secondary...
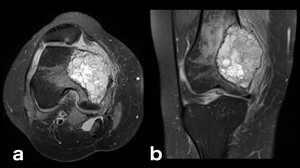
: tumorigenic edema is also present.")
Fig. 23:
Giant Cell Tumor (PD-FS-WI): tumorigenic edema is also present.
.")
Fig. 24:
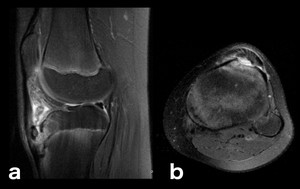
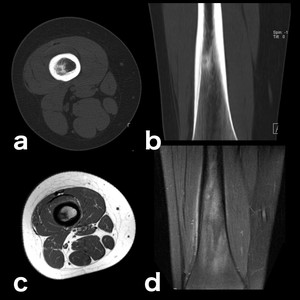
Osteoid Osteoma: in these benign tumors edema can be secondary to an induced...
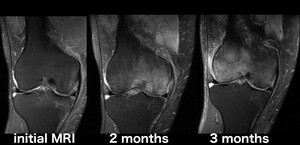
: sagittal intermediate-weighted fat-suppressed MR image of a 30-year-old woman with acute knee pain shows bone marrow edema involving the non-weight-bearing area of the lateral femoral condyle, which underwent almost complete spontaneous resolution over the course of 1 year. Transient Bone Marrow Edema Syndromes are self-limiting entities which manifest as arthralgia associated with bone marrow edema evidence on MRI studies.[8] Its etiology remains uncertain.[8]")
Fig. 25:
Transient Bone Marrow Edema Syndrome (Transient Osteoporosis): sagittal...
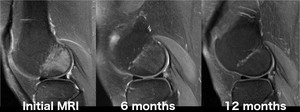
 (serial coronal PD-FS-WI): In some cases a location shift of the bone marrow edema is seen on serial MRIs, this is known as Regional Migratory Osteoporosis (RMO).[8] Although it’s more common to witness a spontaneous resolution of the transient bone marrow edema syndrome, a shift to a different joint can occur in a small fraction of cases, or (even rarer) a shift to a different site within the same articulation (i.e. intra-articular shifting), as seen on this patient.[8] On this intra-articular RMO case there was no trauma history, the edema started on the medial femoral condyle and 3 months later the findings had shifted to the lateral condyle.")
Fig. 26:
Regional Migratory Osteoporosis (a Transient Bone Marrow Edema Syndrome with...
: the confluent and patchy moderately hyperintense pattern here shown in all sequences on the epiphysis is typical of transient osteoporosis following prolonged immobilization. Resuming activity produces bigger stress in the disused bone than in the normal bone because the trabeculae, which have to support the load, are less and weaker, hence bone edema ensues (a stress reaction is also seen on the medial condyle and marked with an *).[7] An healed lateral tibial plateau fracture, responsible for the immobilization, is also apparent (arrow). (a-e: PD-FS-WI; f: T1-WI). It’s also worth noting that Complex Regional Pain Syndrome (CRPS, comprehending the terms reflex sympathetic dystrophy, algoneurodystrophy, and Sudeck’s atrophy) has the same MRI bone edema pattern as DO but it’s pathophysiology is not related to disuse demineralization and it’s always painful (DO is an incidental finding in an asymptomatic patient with known immobilization history).[8]")
Fig. 27:
Disuse Osteoporosis (DO): the confluent and patchy moderately hyperintense...