Bone marrow edema represents an increase in interstitial fluid,
as such it has the MR characteristics of increased water content,
namely a low/intermediate signal on T1-weighted images and a high signal on T2 and PD-weighted images.[2] Water sensitive sequences such as short-tau inversion recovery (STIR) imaging are very sensitive in detecting bone marrow edema as it appears hyperintense compared with normal bone marrow.[3]
Following intravenous gadolinium administration minimal delayed enhancement can be seen with marrow edema,
particularly in the vasogenic forms (as explained ahead).[2]
In contrast to stroke,
posttraumatic marrow edema is associated with increased diffusion on DWI (diffusion weighted-imaging) sequences.[2]
As stated above,
marrow edema results from excessive fluid accumulation in the extracellular space,
and its MR presentation is rather characteristic,
but one should be aware that the same MRI findings can also represent areas of necrosis and/or hemorrhage.[2]
Several mechanisms can be involved in the pathophysiology of bone edema.
We follow the division proposed by Eustace[1]: hyperemic/vasogenic,
congestive,
tumorigenic,
traumatic,
and an atypical group.
We’ve reordered them according to incidence,
arranged some of the rarer and less consensual entities into the Atypical/Others group (even though some of their mechanisms could fit elsewhere) and named the Traumatic/Degenerative group as such to reflect the microtraumatic nature of the traditionally degenerative classification of osteoarthritis:
1.
Traumatic/Degenerative
- Trauma is the most common cause of bone marrow edema.[2] Direct trauma causes immediate disruption of the trabeculae with seepage of interstitial fluid and hemorrhage into the extracellular space.
In traumatic bone edema (commonly referred to as a bone bruise, contusion or trabecular microfractures[4]) the cortex remains intact, while in a true fracture the overlying cortex is disrupted.[2]
2.
Congestive
- Impaired removal of fluid can lead to increases in hydrostatic pressure at the capillary bed resulting in leakage to extravascular spaces.
Congestion typically results from vascular occlusion or thrombosis either idiopathic (e.g. avascular necrosis) or secondary to other causes of elevated marrow space pressures as in hemoglobinopathies,
marrow packing disorders,
fat cell hypertrophy or steroids use.[2]
3. Hyperemic/vasogenic
- Increased delivery of blood and serum to the marrow capillary bed (with or without changes in permeability) will lead to an increased accumulation of interstitial fluid.
This is promptly identified at or adjacent to sites of inflammation due to infection,
along the margins of joints affected by acute synovitis,
and in patients with posttraumatic reflex sympathetic dystrophy.[2]
4. Tumorigenic
- Similar mechanism to the congestive capillary leakage.
Most tumorigenic edema is a consequence of direct capillary trauma from trabecular destruction with the release of intravascular fluid and associated hemorrhage.
Its presence is an indirect marker of malignancy.
In a minority of cases,
edema is instead secondary to an induced inflammatory response (most commonly in osteoid osteomas via prostaglandin E2).[2]
Bone marrow contusions (which can result either from direct blow to the bone,
from compressive forces of adjacent bones impacting one another,
or from traction forces that occur during an avulsion injury) typically have a distribution that reflects the mechanism of trauma: five contusion patterns are well described:[3]
- Pivot Shift Injury
- Dashboard Injury
- Hyperextension Injury
- Clip Injury
- Lateral Patellar Dislocation
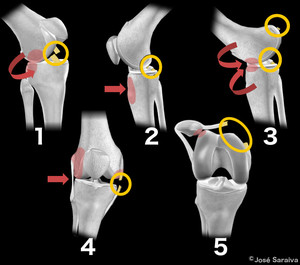
Fig. 1: 1) Pivot Shift Pattern (e.g. skiing accident): involves the posterolateral tibial plateau and the midportion of the lateral femoral condyle. ACL tear is frequently associated. 2) Dashboard Pattern (e.g. car accident): edema on the anterior aspect of the proximal tibia. PCL tear is frequently associated. 3) Hyperextension Pattern (e.g. soccer lesion): “kissing” contusion pattern involving the anterior aspect of the proximal tibia and distal femur. PCL tear is also frequently associated. 4) Clip Injury Pattern (e.g. rugby tackle): large area of edema involving the lateral femoral condyle and a smaller area on the medial femoral condyle. Medial Collateral Ligament (MCL) injuries can be associated. 5) Lateral Patellar Dislocation: edema involving the inferomedial patella and anterior aspect of the lateral femoral condyle. Medial Patellofemoral Ligament (MPFL) is frequently disrupted (see case ahead).
References: José Saraiva
Examples and further considerations on mechanisms 1,
4 and 5 (pivot shift injury,
clip injury and lateral patellar dislocation) can be appreciated on the "Findings and procedure details" section (1: Fig. 9, Fig. 10; 4: Fig. 11; 5: Fig. 8).
These localized patterns are among the most characteristic presentations of bone marrow edema around the knee.
When the edema is diffuse it’s more challenging to find the correct cause,
and sometimes the patient and attending physician are not able to provide clues prior to imaging.
Transient osteoporosis,
neuromuscular dysfunctions,
neoplastic bone lesions or even minor trauma can be unknown at the time of the MRI scan.
In the absence of trauma history and no other discernible cause for the finding of diffuse edema,
transient bone marrow edema syndromes can be diagnosed.

 Pivot Shift Pattern (e.g. skiing accident): involves the posterolateral tibial plateau and the midportion of the lateral femoral condyle. ACL tear is frequently associated. 2) Dashboard Pattern (e.g. car accident): edema on the anterior aspect of the proximal tibia. PCL tear is frequently associated. 3) Hyperextension Pattern (e.g. soccer lesion): “kissing” contusion pattern involving the anterior aspect of the proximal tibia and distal femur. PCL tear is also frequently associated. 4) Clip Injury Pattern (e.g. rugby tackle): large area of edema involving the lateral femoral condyle and a smaller area on the medial femoral condyle. Medial Collateral Ligament (MCL) injuries can be associated. 5) Lateral Patellar Dislocation: edema involving the inferomedial patella and anterior aspect of the lateral femoral condyle. Medial Patellofemoral Ligament (MPFL) is frequently disrupted (see case ahead). References: José Saraiva")