ECR 2018 / C-2561
The role of ultrasound in testicular torsion: are there any reliable imaging signs?
Congress:
ECR 2018
Poster Number:
C-2561
Type:
Educational Exhibit
Keywords:
Acute, Outcomes analysis, Ultrasound, Genital / Reproductive system male
Authors:
E. O'Dwyer1, C. O Brien2, A. Heaney2, C. Shortt3; 1 Dublin 24/IE, 2Dublin/IE, 3Carrick-on-Shannon. Co. Leitrim/IE
DOI:
10.1594/ecr2018/C-2561

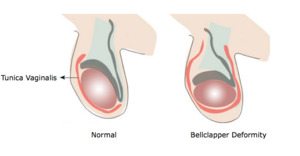
Fig. 1:
Bellclapper Deformity

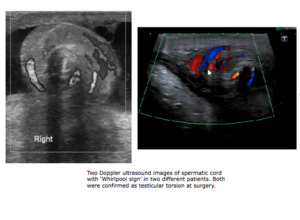
Fig. 2:
Whirlpool Sign

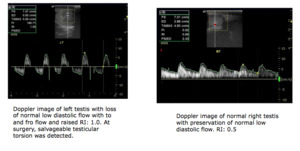
Fig. 3:
Flow abnormality

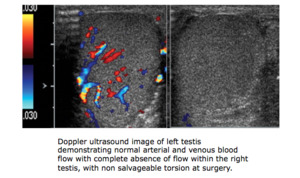
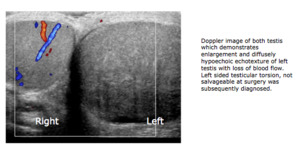
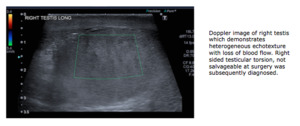
Fig. 4:
Complete loss of flow

Fig. 5:
Alteration of parenchyma

Fig. 6:
Alteration of parenchyma