MRI PROTOCOLS FOR ACUTE APPENDICITIS
In recent literature,
many scanning protocols have been described.
They usually differ only by minor changes,
such as the addition of some specific sequences,
use of different fat suppression methods or use of a different amount of scanning planes.
Regardless the differences,
they all have a quite similar structure,
which represents the backbone of this protocol.
The main scanning protocol for acute appendicitis usually includes:
- T1–weighted images in axial plane
- T2–weighted imaging with single-shot fast spin echo (HASTE,
SSFSE) in axial and coronal planes (sagittal plane is optional)
- T2–weighted images with fat suppression in axial plane (coronal plane is optional)
- Optional: Diffusion-weighted imaging (DWI) in axial plane (coronal plane is optional)
- Optional: T1–weighted images after intravenous contrast media administration in axial plane (coronal plane is optional)
Diffusion-weighted imaging (DWI) and intravenous contrast media administration are,
as already stated above,
optional.
Many instances do not use contrast media in their protocols,
especially while addressing the pediatric and gravid population.
The added value of enhanced MRI in evaluating the appendix and its surroundings is well known,
especially if an abscess is present.
However,
it should be used with caution because of its yet unknown long-term effects.
DWI is also a helpful tool for assessing the area of interest,
giving additional information about the pathology,
but not indispensable.
The sequences can be obtained in a breath-holding manner or in shallow breathing,
depending on the sequence type.
The fast spin echo and other fast sequences have greatly shortened the scanning time,
which is usually less than 20 min.
Sedation,
anesthesia,
bowel relaxant and oral contrast media are not usually given.
The preferred MRI machines for scanning are 1.5 T and 3 T.
Lower Tesla machines will have a worse image quality,
which might compromise the diagnosing process.
MRI CHARACTERISTICS OF NORMAL APPENDIX
A normal appendix is a tubular structure arising from the cecum,
with a diameter measuring 6 mm at most and with a wall thickness of less than 2 mm (Fig. 1).
It has different anatomical positions.
An appendix with retrocecal,
presacral and low pelvic position is harder to find,
especially with US (Fig. 2).
It has a low to intermediate signal intensity on all sequences,
similar to the intensity of the surrounding bowel (cecum and ileum).
The lumen can be collapsed or filled with air or fluid.
Usually,
it has low luminal signal intensity on T1- and T2-weighted sequences,
depending on content.
No periappendiceal changes are present.
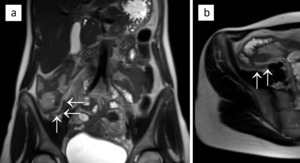
Fig. 1: Image of a normal appendix. T2-weighted images in coronal (a) and axial (b) plane are showing a normal-appearing appendix (arrows), which is not enlarged and shows no inflammatory changes. The appendiceal wall is of low signal intensity, similar to the adjacent bowel wall.
References: Department of Radiology, Izola General Hospital, Slovenia.
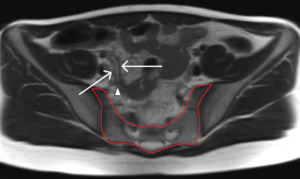
Fig. 2: T2-weighted image shows a normal-appearing appendix with a presacral position. The appendix (arrows) is laying low in the pelvic region; the appendiceal tip (arrowhead) is pointing towards the sacrum (encircled in red).
References: Department of Radiology, Izola General Hospital, Slovenia.
MRI CRITERIA FOR APPENDICITIS
The main MR criteria for appendicitis are:
- enlarged appendiceal diameter (>7mm),
- thickened appendiceal wall (>2mm),
- high-signal-intensity luminal contents on T2-weighted sequences,
- periappendiceal inflammatory changes (hyperintense fat stranding,
fluid collection,
phlegmon,
abscess),
- appendicolith (usually low signal intensity on all sequences,
focal signal void sign),
- restricted diffusion (of appendiceal wall,
appendiceal lumen or focal fluid collection),
- abnormal wall enhancement on post-contrast sequences.
An enlarged appendix with a diameter of more than 7 mm (measured from the outer to outer wall) is suggestive of acute appendicitis (Fig. 3).
In appendices measuring 6-7 mm,
the diagnosis is unclear,
and we should look for periappendiceal pathological changes suggestive of an inflammation (Fig. 4).
If they are present,
the diagnosis of acute appendicitis is very likely.
At this point,
it should be emphasized to always assess the surrounding bowel.
Inflammatory or infective processes affecting primarily the terminal ileum or cecum can spread to the appendix and cause inflammation – the appendix may have an enlarged diameter with a hypervascular and thickened appendiceal wall.
Vice versa,
acute appendicitis can affect the surrounding cecum and terminal ileum,
causing reactive inflammatory changes of the bowel wall.
Sometimes it can be hard to distinguish between these two entities,
but accompanying pathological changes,
disease extent,
laboratory values and a clinical report should help in making the right diagnosis.
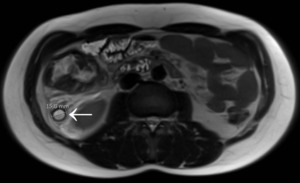
Fig. 3: Acute appendicitis in a 17-year-old male. T2-weighted image in axial plane shows an inflamed, enlarged and fluid-filled appendix (arrow) with a diameter of nearly 16 mm; periappendiceal fat stranding is seen as well.
References: Department of Radiology, Izola General Hospital, Slovenia.
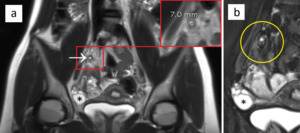
Fig. 4: Ambiguous appendiceal diameter. A 14-year-old female presented to the ED with right-lower quadrant abdominal pain. MRI showed an enlarged appendix (a, arrow) with a diameter of 7 mm. On T2-weighted image with fat suppression (b), the appendix and the periappendiceal region (yellow circle) show no hyperintense inflammatory changes. Acute appendicitis was excluded. A concurrent finding - an ovarian cyst (asterisk), was thought to be the main cause of pain. The patient was discharged after 1 day and she had no further episodes of pain in the following months.
References: Department of Radiology, Izola General Hospital, Slovenia.
The appendiceal wall measuring more than 2 mm is defined as thickened.
The degree may vary,
based on wall hypervascularity and edema.
Because of these inflammatory changes,
the signal of the appendiceal wall will change.
On T1-weighted sequences,
the wall will be of low signal intensity (darker than the normal wall) and on T2-weighted sequences,
it will be of high signal intensity,
representing edema (Fig. 5).
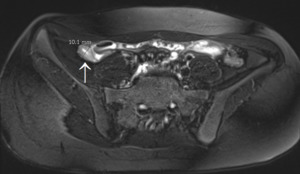
Fig. 5: Edematous acute appendicitis in a 13-year-old female. On T2-weighted image with fat suppression, an inflamed and enlarged appendix is seen (arrow) with a diameter of more than 10 mm. The hyperintense appendiceal wall is thickened (more than 3 mm), representing edema.
References: Department of Radiology, Izola General Hospital, Slovenia.
The high-signal-intensity luminal content on T2-weighted sequences is due to edema or fluid.
Sometimes fluid might be present in a normal-appearing appendix.
This finding alone is not suggestive of inflammation and should not be mistaken for acute appendicitis (Fig. 6).
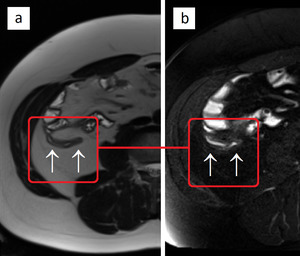
Fig. 6: A fluid-filled normal appendix (arrows). T2-weighted images without (a) and with fat suppression (b) show no periappendiceal inflammatory changes, excluding acute appendicitis.
References: Department of Radiology, Izola General Hospital, Slovenia.
Periappendiceal inflammatory changes consist of hyperintense fat stranding,
fluid collection,
phlegmon and abscess formation.
On T2-weighted sequences with fat suppression,
a high signal of different intensity and extent will be seen in the periappendiceal area (Fig. 7).
Abscess formation can be easier identified on DWI sequences and T1-weighted sequences after intravenous contrast administration.
On DWI,
restricted diffusion will be present in the abscess area.
On post-contrast T1-weighted sequences,
the wall surrounding the abscess will enhance,
demarking the necrotic region.
As the inflammation progresses,
the appendiceal wall may perforate.
In that case,
extensive periappendiceal changes may be seen,
as well as peritonitis and free extraluminal gas.
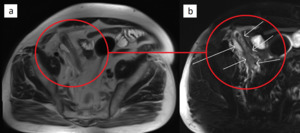
Fig. 7: Acute appendicitis with periappendiceal inflammatory changes in a 64-year-old male (circles). T2-weighted images without (a) and with fat suppression (b) show an enlarged and inflamed appendix (short arrows), periappendiceal fat stranding and a small fluid collection (long arrow). The extent of inflammatory changes is better observed with fat suppression (b).
References: Department of Radiology, Izola General Hospital, Slovenia.
Intra-appendiceal stone or appendicolith is not a common finding.
Usually,
it has a low signal intensity on all sequences (Fig. 8).
On T2-weighted sequences,
where the fluid is bright,
the appendicolith causes a focal signal void (Fig. 9).
This finding alone is not suggestive of appendicitis.
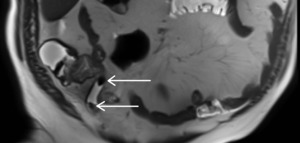
Fig. 8: Two appendicoliths, located in the appendiceal lumen, with a low signal intensity on a T2-weighted image (arrows).
References: Department of Radiology, Izola General Hospital, Slovenia.
Fig. 9: Focal signal void sign on T2-weighted images. The video shows an inflamed and enlarged subhepatic appendix (arrows) with an intraluminal appendicolith in the appendiceal tip; surrounded by fluid, it causes a focal signal void (arrowhead). In the proximal part of the appendix, several dark round formations are seen, representing low-signal-intensity appendicoliths.
References: Department of Radiology, Izola General Hospital, Slovenia.
DWI sequences and post-contrast sequences can be a valuable aid in accessing acute appendicitis.
On DWI sequences restricted diffusion of appendiceal wall,
appendiceal lumen or focal fluid collection can be seen.
While on post-contrast T1-weighted sequences abnormal appendiceal wall enhancement can be identified.
As mentioned earlier,
the abscess wall will enhance,
too.
ALTERNATIVE DIAGNOSIS
Besides acute appendicitis,
many other pathologies can cause acute abdomen and/or pain in the lower abdominal region.
One of the most common are:
- ovarian cyst,
which can (partially) rupture or grow in a short period of time (Fig. 10),
- hemorrhagic ovarian cyst (Fig. 11),
- polycystic ovaries,
seen in young women (Fig. 12),
- mesenteric lymphadenitis,
seen especially in children (Fig. 13),
- terminal ileitis (Fig. 14,
Fig. 15),
- diverticulitis (Fig. 16),
- inflammatory bowel disease (IBD) – Crohn’s disease and ulcerative colitis (Fig. 17,
Fig. 18),
- obstipation and bloating.
Ovarian cysts:
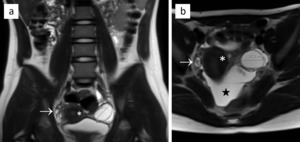
Fig. 10: Ovarian cyst in a 12-year-old female. T2-weighted images in coronal (a) and axial (b) plane show a hyperintense cyst in the left ovary measuring nearly 34 mm. The uterus (asterisk) and the right ovary (arrows) are shown as well. Free intraperitoneal fluid in the pouch of Douglas (star) was a concurrent finding.
References: Department of Radiology, Izola General Hospital, Slovenia.
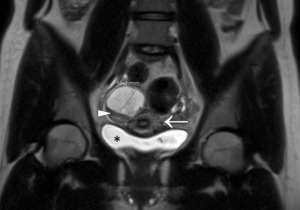
Fig. 11: Hemorrhagic ovarian cyst in a 19-year-old female. T2-weighted image shows a cyst in the right ovary measuring around 45 mm, located adjacent to the uterus (arrow). The fluid inside the cyst is hypointense compared with the fluid inside the urinary bladder (asterisk). Furthermore, a layer of lower signal intensity is seen at the bottom of the cyst (arrowhead). Both characteristics are highly suggestive of a blood-containing ovarian cyst.
References: Department of Radiology, Izola General Hospital, Slovenia.
Polycystic ovaries:
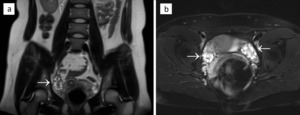
Fig. 12: Polycystic ovaries in a 28-year-old female. T2-weighted images without (a) and with fat suppression (b) show both ovaries (arrows), which contain multiple small hyperintense cysts.
References: Department of Radiology, Izola General Hospital, Slovenia.
Mesenteric lymphadenitis:
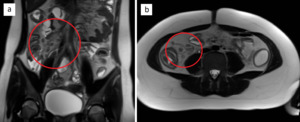
Fig. 13: Mesenteric lymphadenitis in a 12-year-old female. T2-weighted images in coronal (a) and axial (b) plane show multiple enlarged mesenteric lymph nodes, which are best seen in the ileocolic region (circles).
References: Department of Radiology, Izola General Hospital, Slovenia.
Terminal ileitis:
Fig. 14: Terminal ileitis in a 13-year-old male. In this video, consisting of T2-weighted images with fat suppression, the terminal ileum is shown (arrows). While approaching the cecum, the ileal wall progressively thickens, resulting in a high-grade luminal stenosis. Surrounding hyperintense inflammatory changes are seen, as well as free intraperitoneal fluid in the pelvis.
References: Department of Radiology, Izola General Hospital, Slovenia.
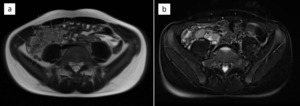
Fig. 15: Terminal ileitis - previous patient (Fig. 14) with additional imaging material: T2-weighted images without (a) and with fat suppression (b). The left image (a) shows multiple grossly enlarged lymph nodes in the ileocolic region (long arrows) and a normal appendix (short arrows). The right image (b) shows an extensively thickened wall of the terminal ileum measuring more than 9 mm. Radiological findings and the clinical report suggested an infectious process.
References: Department of Radiology, Izola General Hospital, Slovenia.
Diverticulitis:
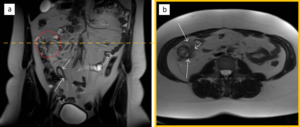
Fig. 16: Diverticulitis in a 46-year-old female. T2-weighted image in a coronal plane (a) shows a normal appendix (arrows) and an inflamed area near the ascending colon (circle). The axial image at the level of the encircled area (b) shows an inflamed and ill-defined diverticulum of the ascending colon (short arrow) with surrounding fat stranding (long arrows), representing diverticulitis.
References: Department of Radiology, Izola General Hospital, Slovenia.
Crohn’s disease:
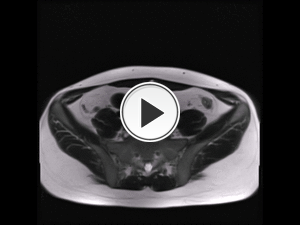
Fig. 17: Crohn’s disease in a 24-year-old male. In this video, consisting of T2-weighted images, the terminal ileum is shown (long arrows). While approaching the cecum (asterisk), the ileal wall progressively thickens, resulting in luminal stenosis. In the surroundings of the thickened wall, extensive fat stranding is seen (short arrows). Further diagnostics and additional MR imaging in the following months confirmed the diagnosis of Crohn’s disease.
References: Department of Radiology, Izola General Hospital, Slovenia.
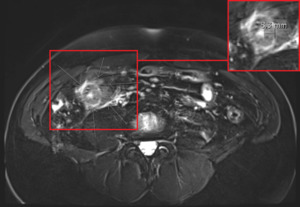
Fig. 18: Crohn’s disease - previous patient (Fig. 17) with additional imaging material. T2-weighted image with fat suppression shows the terminal ileum with an extensively thickened wall, measuring more than 8 mm (square), and surrounding hyperintense inflammatory changes (arrows).
References: Department of Radiology, Izola General Hospital, Slovenia.
MRI ADVANTAGES AND DISADVANTAGES
One of the main advantages of MRI is absence of radiation exposure,
which is extremely important in the pediatric and gravid population.
Unlike with US,
retrocecal appendix,
obese patients and abdominal bloating are no obstacles (Fig. 19).
Further adjustments of MRI protocols have improved the image quality,
lessened the artifacts and noticeably shortened the scan time.
Consequently,
sensitivity and specificity for pathologic processes have increased.
Finally,
yet importantly,
MRI is painless.
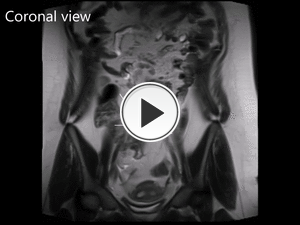
Fig. 19: A 14-year-old and overweight female with a hidden appendix, which could not be identified with the US examination. The following MRI revealed a noninflamed appendix (arrows), bent in the form of a “piggy tail” and with a presacral position. An extensive fat layer and the presacral position were important obstacles for US, but not for MRI.
References: Department of Radiology, Izola General Hospital, Slovenia.
The disadvantages include motion artifacts (breathing,
patient and bowel motion),
need for anesthesia in small children,
relative unavailability (late hours,
no available radiographers) and a higher price compared to CT or US.
An important obstacle to perform MRI is patient’s claustrophobia and the presence of absolute contraindications (metal foreign bodies,
incompatible implants etc.).

 and axial (b) plane are showing a normal-appearing appendix (arrows), which is not enlarged and shows no inflammatory changes. The appendiceal wall is of low signal intensity, similar to the adjacent bowel wall. References: Department of Radiology, Izola General Hospital, Slovenia.")
 is laying low in the pelvic region; the appendiceal tip (arrowhead) is pointing towards the sacrum (encircled in red). References: Department of Radiology, Izola General Hospital, Slovenia.")
 with a diameter of nearly 16 mm; periappendiceal fat stranding is seen as well. References: Department of Radiology, Izola General Hospital, Slovenia.")
 with a diameter of 7 mm. On T2-weighted image with fat suppression (b), the appendix and the periappendiceal region (yellow circle) show no hyperintense inflammatory changes. Acute appendicitis was excluded. A concurrent finding - an ovarian cyst (asterisk), was thought to be the main cause of pain. The patient was discharged after 1 day and she had no further episodes of pain in the following months. References: Department of Radiology, Izola General Hospital, Slovenia.")
 with a diameter of more than 10 mm. The hyperintense appendiceal wall is thickened (more than 3 mm), representing edema. References: Department of Radiology, Izola General Hospital, Slovenia.")
. T2-weighted images without (a) and with fat suppression (b) show no periappendiceal inflammatory changes, excluding acute appendicitis. References: Department of Radiology, Izola General Hospital, Slovenia.")
. T2-weighted images without (a) and with fat suppression (b) show an enlarged and inflamed appendix (short arrows), periappendiceal fat stranding and a small fluid collection (long arrow). The extent of inflammatory changes is better observed with fat suppression (b). References: Department of Radiology, Izola General Hospital, Slovenia.")
. References: Department of Radiology, Izola General Hospital, Slovenia.")
 and axial (b) plane show a hyperintense cyst in the left ovary measuring nearly 34 mm. The uterus (asterisk) and the right ovary (arrows) are shown as well. Free intraperitoneal fluid in the pouch of Douglas (star) was a concurrent finding. References: Department of Radiology, Izola General Hospital, Slovenia.")
. The fluid inside the cyst is hypointense compared with the fluid inside the urinary bladder (asterisk). Furthermore, a layer of lower signal intensity is seen at the bottom of the cyst (arrowhead). Both characteristics are highly suggestive of a blood-containing ovarian cyst. References: Department of Radiology, Izola General Hospital, Slovenia.")
 and with fat suppression (b) show both ovaries (arrows), which contain multiple small hyperintense cysts. References: Department of Radiology, Izola General Hospital, Slovenia.")
 and axial (b) plane show multiple enlarged mesenteric lymph nodes, which are best seen in the ileocolic region (circles). References: Department of Radiology, Izola General Hospital, Slovenia.")
 with additional imaging material: T2-weighted images without (a) and with fat suppression (b). The left image (a) shows multiple grossly enlarged lymph nodes in the ileocolic region (long arrows) and a normal appendix (short arrows). The right image (b) shows an extensively thickened wall of the terminal ileum measuring more than 9 mm. Radiological findings and the clinical report suggested an infectious process. References: Department of Radiology, Izola General Hospital, Slovenia.")
 shows a normal appendix (arrows) and an inflamed area near the ascending colon (circle). The axial image at the level of the encircled area (b) shows an inflamed and ill-defined diverticulum of the ascending colon (short arrow) with surrounding fat stranding (long arrows), representing diverticulitis. References: Department of Radiology, Izola General Hospital, Slovenia.")
 with additional imaging material. T2-weighted image with fat suppression shows the terminal ileum with an extensively thickened wall, measuring more than 8 mm (square), and surrounding hyperintense inflammatory changes (arrows). References: Department of Radiology, Izola General Hospital, Slovenia.")