ECR 2018 / C-2796
Black dots in bad brains - narrowing the differential in SWI abnormalities
Congress:
ECR 2018
Poster Number:
C-2796
Type:
Educational Exhibit
Keywords:
Imaging sequences, Education, MR, Neuroradiology brain, CNS, Pathology
Authors:
H. Nejadhamzeeigilani, H. Cliffe, I. Craven, S. Currie; Leeds/UK
DOI:
10.1594/ecr2018/C-2796
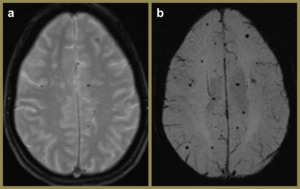
 and SWI (b) images of the same patient at the same level demonstrating the superiority of SWI which is two-fold; a greater number of foci of blooming signal loss reflecting greater sensitivity, and a higher degree of blooming signal loss reflecting greater contrast.")
Fig. 1:
T2* GE (a) and SWI (b) images of the same patient at the same level...
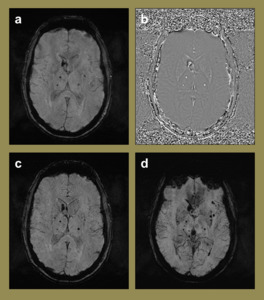
, the phase image (b), the SWI image (c) and the minimum intensity projection (mIP) image (d).")
Fig. 2:
SWI images of a 56-year-old female with a right caudate head haemorrhage and...
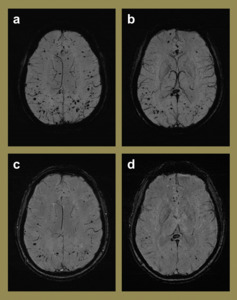
 when compared to the SWI images (c-d) of the same patient at the same level.")
Fig. 3:
Utility of mIP images. Note the ease of detection of numerous microhaemorrhages...