Part I.
SSNs features
I.1 Prevalence
The real prevalence of SSNs it is not directly reported in most of the studies,
therefore is difficult to extract.
As reported in the British Thoracic Society (BTS) Guidelines for the investigation and management of pulmonary nodules,
the PanCan dataset showed that between all the detected nodules the 15.9% were GGNs and the 4.4% were PSNs,
while the BCCA dataset demonstrated a prevalence (between all nodules) of 9.3% and only 0.9% for GGNs and PSNs,
respectively.
By the contrary the I-ELCAP study showed a higher,
albeit slightly,
baseline prevalence of PSNs (5%) compared to GGNs (4.2%),
while at least one solid nodule was found in 30.2%.
A much lower prevalence of SSNs,
with only 0.16% for GGNs and 0.13% for PSNs,
was found in the general population.
In the routine population,
subjects with a SSN appeared to be slightly older (62 years-old vs.
58),
with no gender predilection.
SSNs were mostly located in the upper lobes.
PSNs were larger (1638 vs.
383mm3) and more often progressive (68% vs.
38%) than GGNs,
with progressive SSNs rare under the age of 50 years.
Of course these data cannot be considered as definitive,
with more studied needed,
particularly to establish the prevalence in the general population.
I.2 Malignancy rate and growth rate
Despite the lower prevalence of SSNs than solid nodules both in general and in high-risk population,
they showed a higher malignancy rate,
with the highest prevalence of malignancy associated to PSNs,
followed by GGNs (Table 1).
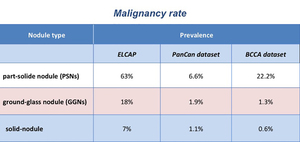
Table 1: Prevalence of malignancy between PSNs, GGNs and solid nodules, respectively, according to three different lung cancer screening trial (data from: Henschke CI et al. (2002) AJR Am J Roentgenol 178:1053–1057; McWilliams A et al (2013) N Engl J Med 369:910–919).
Malignant SSNs have shown mean volume doubling time (VDT) significantly longer than solid nodules,
which is less than 400 days.
In particular,
VDT was calculated to be 813±375 days for GGNs and 457±260 days for PSNs, respectively.
GGNs and PSNs with a solid component of 5 mm or smaller showed significantly longer VDT (mean VDT 1711.2 days) compared to lesions with bigger solid portions (717 days).
Chang at al.
showed that the best predictors of growth where dimension of the nodule and appearance of a solid component.
Anyway most of growing nodules showed an indolent clinical course,
underlining that a strategy of long-term follow-up and selective surgery for growing nodules should be considered.
These evidences underline the need for a longer follow-up for SSNs,
as established in the newer guidelines.
I.3 Predictors of malignancy
A large amount of studies investigates different features of SSNs as predictors of malignancy (Fig. 2).
The most important are:
- initial dimension of the lesion
- growth
- density
- PSN and dimension of solid component
- history of lung cancer
- spiculated margins
- lobulated nodules
- pleural retraction
- bubble-like appearance
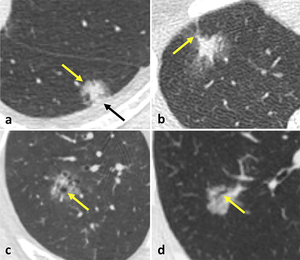
Fig. 2: Predictors of malignancy in SSNs: lobulated borders (a – yellow arrow), pleural retraction (a – black arrow), spiculated margins (b), bubble-like appearance (c), presence of air-bronchogram (d).
As concerning growth,
SSNs can show different growth patterns,
including:
- increase of overall size in GGNs
- diffuse density increase
- development of a solid component in GGNs
- enlargement of the solid component in PSNs
- enlargement of the overall size in PSNs
- both enlargement of the solid component and overall size (Fig. 3).
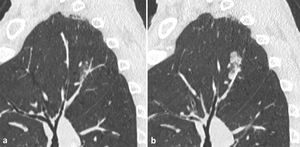
Fig. 3: Evolution (a, b) of a PSN of the upper left lobe in a 63-year-old man, current smoker of 40 pack-year, over a period of 3 years, detected in a lung cancer screening program: both an enlargement of the solid component and of the overall size can be seen. At the histopathological analysis it was demonstrated to be an invasive adenocarcinoma.
Small adenocarcinomas can rarely transiently decrease in size due to peritumoral fibrosis or atelectasis leading to contraction of the nodule.
Some typical radiological patterns,
in terms of both nodule size and density,
can be related to different categories of the adenocarcinoma classification: atypical adenomatous hyperplasia (AAH) and adenocarcinoma in situ (AIS), premalignant and preinvasive lesion,
usually appear as GGNs with a diameter of ≤5mm or >5mm,
respectively; minimally-invasive adenocarcinoma (MIA) as PSN with a solid component <5mm and invasive adenocarcinoma as larger PSN or solid nodule (Table 2).

Table 2: 2011 IASLC/ATS/ERS Classification of Adenocarcinoma, with the different subtypes and their mean CT features.
In PSNs,
the presence of a solid component larger than 5 mm showed a sensitivity of 100% for the detection of invasive adenocarcinoma.
Zhang et al.
found that a diameter of 12.2mm or more,
the presence of solid component of 6.7mm or larger,
the density of the solid component of 192 Hounsfield units (HU) or more were significantly associated with presence of invasive adenocarcinoma.
I.4 Prognosis
Even though SSNs demonstrate a higher malignancy rate than solid ones,
prognosis is good,
with an overall 95-100% 5-years survival after resections.
Histologically,
on CT scan the ground-glass component corresponds to a lepidic pattern,
which is associated to a good prognosis,
while the solid component to invasive growth pattern.
Thus,
the greater the extent of the solid component,
the more likely the lesion will be an invasive adenocarcinoma with an associated poorer prognosis.
For the same reason prognosis better correlates with the diameter of the solid component than on the whole-lesion size. Aoki et al.
demonstrated that PSNs with a ground-glass component larger than 50% had better prognosis.
Dimension of the solid component and presence of air-bronchogram showed to be predictors of lymph-node involvement.
Nodal metastases develop in only less than 1% in case of malignant GGNs.
Due to the low aggressiveness and poor invasiveness of malignant SSNs and the overall good prognosis,
limited resections may be useful,
also taking into account the recurrence risk (especially in patients showing more than one SSNs at baseline CT scan).
I.5 Differential diagnosis
SSNs,
both GGNs and PSNs,
may represent benign and malignant lesions,
being potential expression of infection (including also non-necrotizing granulomata),
inflammation,
focal fibrosis,
haemorrhage and,
of course,
cancer.
Between benign lesions other than infection,
organizing pneumonia,
focal interstitial fibrosis (a focal non-specific pulmonary tissue response to injury,
composed of fibrous thickening of the alveolar walls,
collagen fiber deposition,
anthracosis,
and peribronchovascular interstitial thickening) and pulmonary endometriosis must be taken into consideration for the differential diagnosis.
Between malignant causes the most common lesion showing SSN appearance is lung adenocarcinoma,
but SSNs may also rarely represent metastases, of course solitary or multiple,
from melanoma,
renal cell carcinoma,
and adenocarcinoma of the pancreas,
breast,
and gastrointestinal tract,
or lymphoproliferative disorders such as bronchus-associated lymphoid tissue lymphoma (BALT-oma) (Table 3).
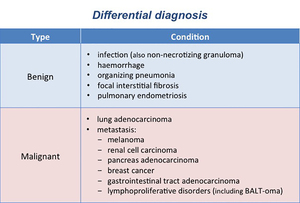
Table 3: Differential diagnosis for SSNs, both GGNs and PSNs, divided into benign and malignant conditions (modified from: Truong MT et al. (2014) RadioGraphics 34:1658-79).
SSNs may be persistent (with persistence assessed at a follow-up CT scan after at least 3 months) or transient.
In fact,
both GGNs and PSNs may be expression of transient infections and may resolve after short-term follow-up (Fig. 4).
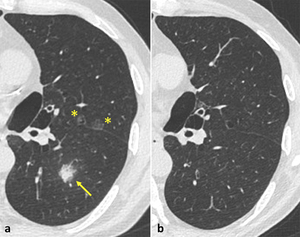
Fig. 4: Baseline CT of a 61-year-old man, current smoker of 90 pack-year, in a lung cancer screening program (a), which demonstrated two small GGNs in the left upper lobe (yellow stars) and a PSN with a solid component of 9 mm (measurement not shown) and ill-defined borders in the left lower lobe. The follow-up after 3 months to confirm the persistence of SSNs showed complete resolution of the findings (b).
Data from I-ELCAP demonstrated that 26% of GGNs and 19.6% of PSNs were transient,
while Oh at al.
showed an even higher percentage of transient nodule,
respectively 37.6% of GGNs and 48.7% of PSNs,
with a prevalence in the PSNs cohort.
Thus,
at least one follow-up CT scan (3–6 months) is recommended to determine persistence or resolution.
Predicting factors of transient SSNs are:
- young age
- male sex
- nodule found at follow-up CT scan
- smoking habit
- peripheral eosinophilia
- multiple nodules
- big lesion/polygonal
- big solid component
- ill-defined borders
By the contrary persistent nodules usually show irregular margins and they are more often associated with pleural retraction and/or air-bronchogram.
Distinguishing between transient lesions and persistent ones is important for patient management,
in order to avoid unnecessary further diagnostic investigations in patients with transient,
thus benign,
nodules.
After a 3-6 months follow-up a persistent PSN is most likely a malignant lesion (either lung adenocarcinoma or metastatic localization),
although the hypothesis of focal interstitial fibrosis cannot be excluded.
I.6 Multiple SSNs
SSNs are frequently multiple.
Patients with multiple SSNs less than 6mm are more likely to have an infection (Fig. 5) and hypothesis other than lung adenocarcinoma have to be excluded first.
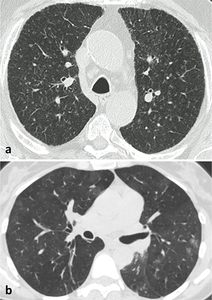
Fig. 5: Benign multiple SSNs. In (a), multiple small GGNs with centrilobular distribution in the upper lobes in a current smoker, suggestive of respiratory bronchilitis. In (b), multiple inflammatory nodules in a young women complaining of cough and dyspnea.
Nevertheless,
multiple SSNs (larger than 6mm) are more likely AAH or AIS,
particularly in women and in never-smokers.
Multiplicity was shown to be a single predictor for benignity,
because most of the nodules appears to be transient or reduces in dimension at follow-up.
Of course,
in case of multiple SSNs in patients with known extra-pulmonary cancer proved to have pulmonary subsolid metastasis,
an important differential diagnosis must be done between multiple pulmonary localizations of multiple primary lung adenocarcinoma.
However,
46.7% of SSNs in patients with extra-pulmonary cancer appeared to be transient after follow-up.
I.7 Measurement
When considering SSNs less than 1cm,
the variability in measuring nodule dimension was found to be lower when using the average diameter than the longest one.
Thus,
the latest statement from the Fleischner Society on nodule measurements supports this evidence and recommends expressing dimension of SSNs <1cm as average diameter (Fig. 6).
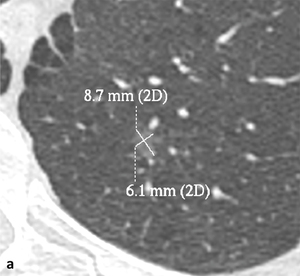
Fig. 6: According to the statement of the Fleischner Society (Bankier AA et al. (2017) Radiology 285: 584–600) the dimension of a small SSN should be expressed as the average diameter of maximal long-axis and perpendicular maximal short-axis measurements in the same plane, both rounded to the nearest millimeter. In the example given, a small GGN, with maximal long-axis of 9 mm and perpendicular maximal short-axis of 6 mm, with a resulting average diameter of 7,5 mm (rounded to 8 mm). 2D: two-dimensional.
Lung window setting shows a comparable reproducibility,
but higher accuracy in SSNs classification and measurement of the solid component than mediastinal window setting.
By the contrary,
with mediastinal window setting,
only areas with density of -160 HU or more can be detected as solid,
resulting in underestimation of the solid portion (Fig. 7).
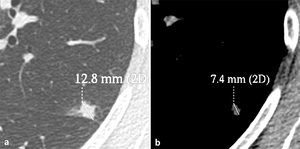
Fig. 7: Image shows the higher accuracy of lung window setting in measuring the solid component of PNSs as compared to mediastinal window setting. By using the lung window setting, the measured maximum axial diameter of the solid portion of the nodule corresponds to 12.8 mm (a), while, by using the mediastinal window, the same diameter corresponds to only 7.4 mm (b). 2D: two-dimensional.
As already underlined,
in PSNs the size of the solid portion correlates with nodule invasive component,
associated with poor prognosis,
as well as the diameter of the solid component better correlate with patient prognosis than the whole-lesion dimension.
For this reason,
the presence and the dimension of different attenuation components within PSNs should be measured and reported.
Therefore,
recommendations of the Fleischner Society suggest the use of lung window setting and high spatial frequency filter to assess the presence of a solid component,
and the measurement of both ground-glass and solid portions in PSNs (Fig. 8).
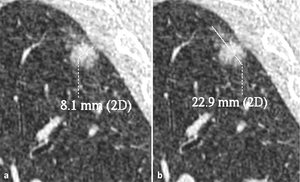
Fig. 8: According to the statement of the Fleischner Society (Bankier AA et al. (2017) Radiology 285: 584–600), in case of PSNs, the maximum diameter of both solid (if >3mm) (a) and ground-glass (b) components should be measured and reported. 2D: two-dimensional.
Part II.
Updated management of SSNs
II.1 Lung cancer screening setting - ACR Lung-RADS
In 2014 the American College of Radiology (ACR) published the Lung-RADS,
a quality-reference tool for reporting standardization of low-dose CT (LDCT) scans in lung cancer screening,
consisting of a system to categorise screening-detected lung nodules.
Its use in the screening setting is nowadays recommended in the recent Fleischner Society Guidelines for incidental nodules.
In Lung-RADS,
nodules are classified according to their morpho-dimensional features,
with an established probability of malignancy.
SSNs,
both GGNs and PSNs,
are specifically framed from category 2 to 4.
Category 4 is in turn divided into A and B and a special category 4X.
Management is distinguished for baseline and follow-up.
Any GGNs <20mm,
GGNs ≥20mm if unchanged or slowly growing after follow-up,
and PSNs with diameter <6mm on baseline are put into category 2,
with malignancy probability <1%.
This category is advised to continue annual screening with LDCT in 12 months.
GGNs ≥20mm on baseline or new at follow-up,
PSNs ≥6mm in total diameter with solid component <6mm or new <6mm in total diameter at follow-up are recommended to perform follow-up with LDCT after 6 months (category 3,
lung cancer probability 1-2%).
PSN ≥ 6mm with solid component from ≥6mm to <8mm or in case of a new or growing solid component <4mm at follow-up are classified as category 4A (malignancy probability 5-15%).
For this category follow-up at 3 months with LDCT is recommended (or PET-CT scan in case of a solid component ≥8mm).
More stringent follow-up using chest CT with or without contrast medium,
PET-CT (in case of a solid component ≥8mm) or tissue sampling is recommended in case of a new or growing PSN with solid component ≥4mm or a baseline PSN with solid component ≥8mm (category 4B,
malignancy probability >15%).
Category 3 and 4 nodules unchanged after follow-up ≥3 months can be downgraded into category 2 (annual LDCT screening) (Table 4).
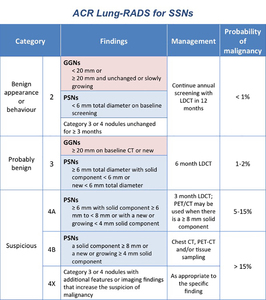
Table 4: Management of screening-detected SSNs according to the ACR Lung-RADS (modified from: American College of Radiology. Lung CT Screening Reporting and Data System (Lung-RADS). www.acr.org/Quality-Safety/Resources/LungRADS Date last accessed May 12, 2016. Date last updated: April 28, 2014).
Nodules assigned to category 3 or 4 can be upgraded to category 4X in case additional features or imaging findings that increase the suspicion of lung cancer (such as spiculation,
GGN that doubles in size in 1 year,
enlarged lymph nodes,
etc.).
The added value of the Lung-RADS category 4X has been evaluated for SSNs in a recent study,
which demonstrates that the malignancy rate derived by adding morphological criteria is superior to the probability assessed only on nodule type and size,
with an average rate of malignancy of 53% (with respect >15% assigned by Lung-RADS).
II.2 Everyday life - Fleischner Society Guidelines for incidental nodules
The new Fleischner Society Guidelines refers to general population of adult patient who are at least 35 years old,
non immunocompromised and without known primary cancers.
Due to the indolent growth of malignant SSNs longer follow-up intervals and total follow-up time lapse are recommended than solid nodules.
For single SSNs <6mm,
both GGNs and PSNs,
follow-up is generally not required,
even if for nodules close to 6mm follow-up at 2 and 4 years may be reasonable when considering factors such as morphology and additional risk-factors.
GGNs ≥6mm should receive a follow-up at 6-12 months to confirm persistence and CT scans every 2 years until 5 years follow-up.
PSNs ≥6mm should receive a follow-up within 3–6 months for persistence,
then annual LDCT scans for 5 years.
Persistent PSNs with a solid component ≥6mm are considered highly suspicious for lung cancer and for this reason resection should be consider.
In case of multiple SSNs,
after initial follow-up at 3-6 months to confirm persistence,
management should be based on the most suspicious nodule.
Multiple GGNs <6mm are usually benign,
but follow-up at 2 and 4 years may be considered in selected patients (Table 5).
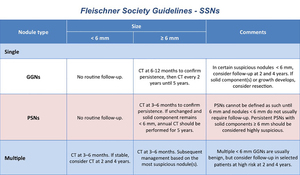
Table 5: Management of SSNs in the general population according to the Fleischner Society Guidelines (modified from: MacMahon H et al. (2017) Radiology 284:228–243).

 AJR Am J Roentgenol 178:1053–1057; McWilliams A et al (2013) N Engl J Med 369:910–919).")
, pleural retraction (a – black arrow), spiculated margins (b), bubble-like appearance (c), presence of air-bronchogram (d).")
 of a PSN of the upper left lobe in a 63-year-old man, current smoker of 40 pack-year, over a period of 3 years, detected in a lung cancer screening program: both an enlargement of the solid component and of the overall size can be seen. At the histopathological analysis it was demonstrated to be an invasive adenocarcinoma.")

 RadioGraphics 34:1658-79).")
, which demonstrated two small GGNs in the left upper lobe (yellow stars) and a PSN with a solid component of 9 mm (measurement not shown) and ill-defined borders in the left lower lobe. The follow-up after 3 months to confirm the persistence of SSNs showed complete resolution of the findings (b).")
, multiple small GGNs with centrilobular distribution in the upper lobes in a current smoker, suggestive of respiratory bronchilitis. In (b), multiple inflammatory nodules in a young women complaining of cough and dyspnea.")
 Radiology 285: 584–600) the dimension of a small SSN should be expressed as the average diameter of maximal long-axis and perpendicular maximal short-axis measurements in the same plane, both rounded to the nearest millimeter. In the example given, a small GGN, with maximal long-axis of 9 mm and perpendicular maximal short-axis of 6 mm, with a resulting average diameter of 7,5 mm (rounded to 8 mm). 2D: two-dimensional.")
, while, by using the mediastinal window, the same diameter corresponds to only 7.4 mm (b). 2D: two-dimensional.")
 Radiology 285: 584–600), in case of PSNs, the maximum diameter of both solid (if >3mm) (a) and ground-glass (b) components should be measured and reported. 2D: two-dimensional.")
. www.acr.org/Quality-Safety/Resources/LungRADS Date last accessed May 12, 2016. Date last updated: April 28, 2014).")
 Radiology 284:228–243).")