Type:
Educational Exhibit
Keywords:
Neoplasia, Cancer, Screening, Education, CT-High Resolution, CT, Thorax, Oncology, Lung
Authors:
G. Cicchetti1, A. Farchione1, P. Franchi1, D. Geat1, G. Sica1, A. del Ciello2, A. R. Larici1, L. Bonomo1, R. Manfredi1; 1Rome/IT, 2Roma/IT
DOI:
10.1594/ecr2018/C-2807
Background
As everybody knows,
a pulmonary nodule is a rounded opacity,
well or poorly defined,
measuring up to 3cm in diameter.
In this definition are included both solid nodules and SSNs.
However,
this poster is focused on SSNs and solid nodules will not be discussed.
SSNs can be distinguished into two main categories:
- pure ground-glass nodules (GGNs), which are nodules characterized by hazy increased lung attenuation,
that does not obliterate the bronchial and vascular margins;
- part-solid nodules (PSNs),
which contain both ground-glass and solid soft-tissue attenuation components (Fig. 1).
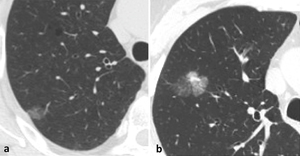
Fig. 1: Figure shows a ground-glass nodule (GGN) (a) and a part-solid nodule (PSN) (b).
According to the recent Fleischner Society Guidelines,
in practice,
PSNs cannot be defined as such until 6mm in diameter because discrete solid components cannot be reliably defined.
SSNs show a very variable and much wider morphological spectrum than solid nodules,
whose corresponds to different predictors in term of malignancy and prognosis.
For this reason,
criteria for the evaluation and management of SSNs are still in becoming and non-unique.
Lung cancer screening programs have allowed collecting a large amount of data about SSNs features,
by analysing large populations of high-risk subjects.
However,
everyday clinical practice and lung cancer screening setting must be always considered separately,
because of the different risks of malignancy between patients belonging to these different categories,
considering different managements and applying specific guidelines.

 (a) and a part-solid nodule (PSN) (b).")