1.
Gallbladder wall thickening
The normal gallbladder wall appears as a pencil-thin echogenic line on sonography.
A thickened gallbladder wall measures more than 3 mm,
and typically has a layered appearance at sonography (1).
Differential diagnosis of diffuse gallbladder wall thickening:
- Cholecystitis (acute; chronic; acalculous; xanthogranulomatous)
- Direct inflammatory spread from adjacent structures (pancreatitis; hepatitis; pyelonephritis)
- Systemic disease (Heart failure; Kidney failure; Chronic hepatic disease; Sepsis)
- Carcinoma
- Hyperplastic changes (adenomyomatosis)
In some cases, pseudothickening is mentioned because the thickness of the GB wall depends on the degree of gallbladder distention.
Pseudothickening can occur in the postprandial state due to physiologic contraction (2).
The diffuse thickening of the GB wall can be seen in patients whom the GB is secondary involved in an extrinsic pathological condition,
such as inflammatory spread of adjacent structures or systemic diseases.
Systemic diseases like heart or kidney failure,
may cause low intravascular osmotic pressure or elevated portal venous pressure possibly related to the thickening of the GB wall (2).
(Fig.
1)

Fig. 1: Ultrasound image showing GB wall thickening in a pacient with heart failure.
Chronic cholecystitis refers to symptomatic gallbladder stones that cause transient obstruction,
leading to a low-grade inflammation with fibrosis (1).
Correlation of findings like gallstone with slightly thick GB wall and clinical history is essential to a correct diagnosis.
-
Xanthogranulomatous cholecystitis is an unusual variant of chronic cholecystitis,
probably induced by intramural extravasation of bile from the Rokitansky-Aschoff sinuses or from superficial mucosal ulcerations,
leading to an inflammatory response in which histiocytes predominate as they ingest the chemically irritating cholesterol crystals.The presence of multiple intramural hypoechoic nodules or bands is typical.
Gallstones are often present.
Adenomyomatosis of the GB is a hyperplastic cholecystosis of the gallbladder wall with intramural diverticula (Rokitansky-Aschoff sinuses),
it is a relatively common and benign cause of diffuse or focal GB wall thickening.
Current thinking is that adenomyomatosis is not premalignant but may be seen in chronically inflamed gallbladders,
which have a higher risk for developing cancer (1).
Ultrasound findings of ‘comet-tail’ reverberation artifact in a thickened GB wall suggests this diagnosis.
(Fig.
2)

Fig. 2: Ultrasound images showing ‘comet-tail’ reverberation artifact of adenomyomatosis.
The GB carcinoma is the fifth most common malignancy of the gastrointestinal tract,
and is found incidentally in 1% to 3% of cholecystectomy specimens (4).
Cholelithiasis is a risk factor for developing gallbladder carcinoma,
and gallstones are present in about 80% of cases (2).
Ultrasound findings that are related with malignancy include heterogeneous irregular wall thickening and an extraluminal mass extending into the liver. (Fig.
3)
2. Sonographic features and pathophysiology of acute cholecystitis
AC is the most frequent inflammatory condition of the GB.
The presence of cholelithiasis in combination with a positive sonographic Murphy sign is highly specific for AC.
(2)
Approximately 10-15% of people in the Western hemisphere have cholelithiasis (5).
90-95% of cases of AC are associated with cholelithiasis causing obstruction of the cystic duct or GB neck (6).
(Fig.
4)
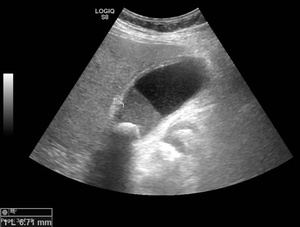
Fig. 4: Ultrasound image showing acute calculous cholecystitis with diffuse gallbladder wall thickening. Gallstone impacted on GB neck. Liquid-liquid level representing sludge in the dependent portion.
Ultrasound findings on acute cholecystitis
- Gallstone or sludge
- Positive sonographic murphy sign
- Wall thickened (> 3 mm)
- Pericholecystic fluid
- GB distended (>4 cm transverse; >10 cm longitudinal)
Acalculous cholecystitis occurs most often in critically ill patients.
This condition is thought to be due to a gradual increase in bile viscosity that eventually leads to functional obstruction of the cystic duct with bile stasis (2).
Ultrasound features are the same of AC apart from cholelithiasis.
(Fig.
5)
3.
Pathophysiology of cholecystitis
The main symptom of cholelithiasis is biliary colic,
which occurs when a stone obstructs the cystic acutely,
leading to a sudden expansion with increased pressure in the gallbladder that results in pain.
This is the most frequent cause of right upper quadrant abdominal pain.
Its persistence in time,
should make us think of acute cholecystitis.
The degree of obstruction and the duration of the obstruction are the two factors which determine the progression to AC (7).
As time goes by,
there is a progressive ductal ectasia,
more chemical irritation of the mucosa and finally wall ischemia,
considering the infection as a secondary phenomenon.
If the patient does not receive early treatment,
the disease becomes more serious and complications occur (7).
Pathologically,
there are three stages of inflammatory disease: (a) oedematous cholecystitis; (b) necrotising cholecystitis; and (c) suppurative cholecystitis (7).
a - edema in the subserosal layer,
gallbladder tissue remains intact
b - areas of hemorrhage and necrosis,
does not involve the full thickness of the GB wall
c - gallbladder begins to contract and the wall is thickened due to fibrous proliferation,
intrawall abscesses are present.
4.
Complicated acute cholecystitis
Secondary bacterial infection is present in 20% of cases of acute cholecystitis.
Mural ischaemia resulting from the increased intraluminal pressure may also contribute to complications such as gangrenous cholecystitis and perforation.
(8) Others complications are emphysematous cholecystitis and haemorrhagic cholecystitis.
4.1 Cholecystitis gangrenous
Refers to ischaemia with necrosis of the gallbladder wall,
it’s the most common complication of AC (9).
Risk factors: male; increasing age; delayed surgery; cardiovascular disease; diabetes mellitus.
Occurs in up to 39% of patients with acute calculous cholecystitis (10).
Ultrasound features: (Fig.
6)
- Hyperechoic linear structures within the lumen
- Striated pattern between hyperechoic and hypoechoic bands
- Asymmetric wall thickness
- Focal perfusion defects on Doppler
4.2 Cholecystitis emphysematous (Fig.
7)
- Most common in diabetic patients (2).
- Dirty shadowing (intramural gas).
- CT is considered the most sensitive and specific imaging modality for identifying gas within the gallbladder lumen or wall (11).
4.3 Gallbladder perforation - result of ischemia and necrosis of the gallbladder wall,
more commonly associated with gangrenous cholecystitis.
Ultrasound features includes pericholecystic fluid collection(s) with a layering of the gallbladder wall (12).
(Fig.
8)
Cholecystoenteric fistula – consequence of chronic perforation,
usually presents communication with duodenum.
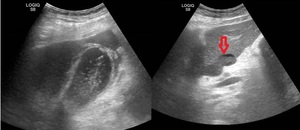
Fig. 8: Ultrasound images showing GB perforation. Red arrow - abscess adjacent to liver left lobe.
4.4 Haemorrhagic cholecystitis (Fig.
9)
- Risk factors: bleeding diathesis or treatment with anticoagulants
- Ultrasound features: mixed echogenicity non-shadowing material filling the lumen; signs of AC may be present.
Gallstones may not be apparent due to the intraluminal blood.
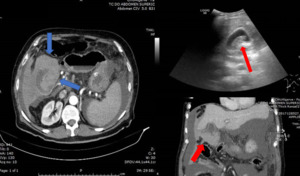
Fig. 9: Ultrasound image showing ecogenic content within the lumen of the GB and CT images showing perforation of GB with slightly hyperdense content inside the GB. After surgery the diagnosis was Hemoperitoneum with GB perforation.









