The GCA is the systemic vasculitis more predominant in adults.
The blood vessels of large-medium caliber more frequently involved are the aorta,
subclavican and iliac arteries,
with predilection for the coronary and vertebral arteries.
The GCA is also known as Temporal Arteritis,
due to its predilection for the temporal arteries,
small caliber blood vessels which are involved in the majority of patients.
It is also known as Horton's syndrome,
arteritis of the aged or granulomatous arteritis.
There are various etiological factors acknowledge as being predisposing factors of GCA and a well known association with Polymyalgia Rheumatica.
It affects predominantly the female sex and people over 50 years of age,
reaching its peak between the ages of 70-80 years.
In Europe it is more prevalent in the Nordic countries.
Being a chronic granulomatous inflammation,
it affects the intima,
media and adventitia of the arteries involved,
with infiltration by lymphocytes,
macrophages and giant multinucleated cells.
The parietal involvement does not have to be continuous,
frequently with skip lesions.
The alterations lead to thickening of the wall with subsequent lumen stenosis.
The hallmark is an elevation in the erythrocyte sedimentation rate (ESR) superior to 50mm/h.
It is necessary to present with at least three of the classification criteria of the American College of Rheumatology (ACR). (table2)
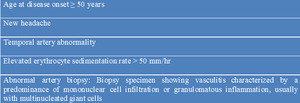
Table 2: Diagnostic Criteria for Giant Cell Arteritis according to the American College of Rheumatology.
Temporal artery biopsy is the diagnostic gold standard.
Ideally it should be performed before initiating treatment with steroids,
which is not always possible; nonetheless,
it maintains a diagnostic value up to 4-6 weeks. Preferentially,
it should not be done after 2 weeks of initiating treatment.
Ultrasonography of the Temporal Arteries
The color duplex ultrasonography can be utilized to assist in diagnosing GCA,
being the evaluation of the temporal arteries the most commonly performed.
Technique
The ultrasound machines machines used should be of high-quality.
The probes should be linear with ideal frequencies between 10-15 MHz,
but at least with a minimum of 9MHz,
with preset of small parts.
The patient should be lying in a supine position with the head slightly elevated and facing towards the opposite side of the artery being evaluated.
Both of the temporal arteries should be evaluated using longitudinal and transversal scans.
The superficial temporal artery should be scanned starting in the distal portion of the common trunk,
in the region below the ear,
throughout its course until the parietal and temporal ramus (approximately 7-10 cm).
The exam should be initiated in B mode,
evaluating the morphology of the superficial temporal artery and its parietal and temporal branches,
including a measurement of the luminal systolic diameter in the sagittal plane and the parietal thickness.
The blood vessels present with thin and homogenous walls,
with internal regular surfaces.
(figure 1)
The normal diameters of the arteries involved are: in the common superficial temporal artery 1.70+-0.43mm; parietal branch 2.3+-0.38mm and frontal branch 2.2+-0.38mm.
In the examination by color Doppler and spectral/pulsed waved curves,
it is possible to evaluate the arterial flow and its velocities .The steering of the color box should be adequate,
with a corrected angle of 20º-30º when the blood vessel is parallel to the skin.
The pulse repetition frequency should be of 2-2.5 kHZ.
(figure 1)
The blood vessel lumen should be totally filled by the color,
trying to avoid partial,
central,
fillings that underestimate the parietal thickness,
leading to a misdiagnosis such as inflammatory edema.
Blood vessels overfilled by the color obscure the wall and the thickening can be underestimated or be undetected.
The maximum arterial velocities should be measured in at least three segments of the artery:
- Trunk of the common superficial temporal artery,
in front of the tragus (normal:55+13 cm/sec).
- Parietal branch,
at 15 mm bifurcation (normal: 54+14 cm/sec).
- Frontal branch,
at 25 mm bifurcation (normal: 47+15 cm/sec).
Ultrasound can also evaluate the occipital,
vertebral and facial arteries.
The blood vessels of medium and large caliber,
namely the subclavian,
axillary and brachial proximal arteries,
are frequently affected.
It is recommended to do bilateral auscultation of the subclavian and axillary regions,
with bilateral blood pressure measurement.
US of the axillary region should be performed on all patients with strong suspicions of GCA and with Polymyalgia Rheumatica.
Ultrasound can also evaluate the occipital,
vertebral and facial arteries.
The blood vessels of medium and large caliber,
namely the subclavian,
axillary and brachial proximal arteries,
are frequently affected.
It is recommended to do bilateral auscultation of the subclavican and axillary regions,
with bilateral blood pressure measurement .
US of the axillary region should be performed on all patients with strong suspicions of GCA and with Polymyalgia Rheumatica.
Expected pathological features:
The depositing of macrophages on the blood vessel walls stimulates the production of vascular endothelial growth factor (VEGF) which,
in conjunction with the platelet-derived growth factor (PDGF),
stimulate the hyperplasia of the intima in a relatively uniform manner.
This thickening and parietal edema present in the ultrasound B mode as a hypoechoic halo circumferentially around the lumen of the inflamed arteries,
with 0.3 mm to 2 mm. (figure 2 and 3 )
Consequently,
in the regions of thickening of the intima,
the diameter of the blood vessel lumen is reduced.
Stenosis is defined when the blood flow velocity is more than double in this region,
when compared with the segment measured 3-5 mm previous to the stenosis. (figure 2 and 3)
There can be coexistence of turbulence in the wave,
with lower velocity behind the area of stenosis,
or persistence of the color signal during the diastole.
Acute occlusions can occur and are identified when there is hypoechoic material occupying the arterial lumen,
without detected color signals.
(figure 2 and 3)

Fig. 2: Doppler ultrasound of the right superficial temporal artery with a prominent hypoechoic halo in the transverse (A) and longitudinal (B) plans, the last one showing a diminished caliber. Color study and power Doppler (C and D) reveal flux turbulence in the region of diminished caliber , due to an increase bigger than twice the velocity in the pre-stenotic segment.
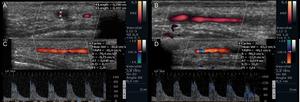
Fig. 3: Same patient, Doppler ultrasound of the left superficial temporal artery with a prominent hypoechoic halo in the transverse (A) and longitudinal (B) plans and also a focal caliber reduction. Color study and power Doppler ( C and D ) reveal flux turbulence in the region of diminished caliber, but without a significant increase of the velocity in the pre-stenotic segment.
Doppler Ultrasound advantages
US is a widely available technique,
non invasive and inexpensive.
With newer and improved equipment,
the results are higher in specificity and sensitivity.
Compared to a temporal artery biopsy,
the halo sign has 75% sensitivity and 83% specificity.
Comparing to ACR criteria,
it presents with 69% sensitivity and 89% specificity.
When the halo sign,
stenosis and occlusion are considered together,
sensitivity is further increased in comparison to biopsy and ACR criteria to 83% and 78%,
respectively.
The halo sign has the highest specificity,
thus,
its presence strongly supports the diagnosis.
The role of US in follow-up is still under discussion.
We know that, with progressive response to therapy, the halo sign diminishes and can disappear in an average of 16 days after initiating corticosteroids.
However,
in the case of inflammatory alterations of the larger arteries,
the edema of the wall will not respond in the same manner,
it can remain for months even years; although with a progressively more echoic appearance.
US has more advantages comparatively to biopsy.
The latter is an invasive procedure,
is not completely innocuous,
is not readily available and the histologic result is influenced by therapy.
Due to the potential of skip lesions,
it can miss the focal point of the illness,
which originates a contralateral biopsy in patients with strong clinical suspicion.
Arteriography permits a morphological evaluation of the temporal arteries,
identifying stenosis or occlusions,
but without sufficient resolution to evaluate the inflammatory alterations of the wall.
High-resolution contrast-enhanced Magnetic Resonance Imaging (MRI) and MR Angiography can demonstrate the temporal arteries as well other arteries such as the aorta, and isolate inflammation of the occipital arteries. However,
its application in evaluating the GCA still needs further exploration.
US is also advantageous in relation to MRI,
with a superior resolution of the inflammatory wall alterations,
as well arteriography,
with which it is not possible to delineate the wall.
Doppler Ultrasound limitations
US is an operator dependent exam.
It is recommended that the radiologist should have performed at least 50 scans of patients without pathology of the temporal arteries.
The sensitivity of the findings is lower than specificity,
namely the halo sign,
thus its absence does not exclude Temporal Arteritis.
Findings are influenced by the treatment,
with disappearance and reappearance of the halo sign,
respectively,
in response to treatment and in relapse.
It should be performed during the first 7 days of treatment.
It does not differentiate from other vasculitis that affect the temporal arteries,
namely Wegener Granulomatosis,
Churg Strauss Syndrome and Microscopic Polyangiitis.
Takayasu Arteritis
Takayasu Arteritis,
also known as Aortoarteritis or pulseless disease,
is a rare systemic vasculitis,
which more frequently involves the blood vessels of large and medium calibre,
with predilection for the aorta and its branchs,
namely the subclavian,
carotid, vertebral and renal arteries.
Being a chronic granulomatous inflammation,
it affects the blood vessel wall in a transmural way.
Lesions can be stenotic,
occlusive or aneurysmatic.
They are classified in accordance with the segments involved.
l Type I - Branches of the aortic arch
l Type IIa - Ascending aorta,
aortic arch,
and its branches
l Type IIb - Type IIa region plus thoracic descending aorta
l Type III - Thoracic descending aorta,
abdominal aorta,
renal arteries,
or a combination
l Type IV - Abdominal aorta,
renal arteries,
or both
l Type V - Entire aorta and its branches
No known cause for this illness has been established.
However,
there are some etiological factors that may be predisposing,
namely,
infections or autoimmune processes.
Although it can affect children,
it affects preferentially females below 50 years of age.
The median age of onset is about 30 years.
This illness is more common in Asia.
The classical presentation of Takayasu Arteritis is not the norm and consists of three phases:
- Early pre-stenotic phase: appearance of non specific,
systemic insidious symptoms.
- Active vascular inflammation phase: Localized pain in the areas affected,
and symptoms of vascular insufficiency.
- Burnout disease: Appearance of fibrotic and stenotic lesions.
For a patient to be classified as having Takayasu Arteritis,
at least three criteria of the American College of Rheumatology have to be present. (table 3)
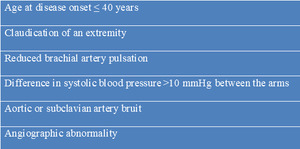
Table 3: Diagnostic Criteria for Takayasu Arteritis according to the American College of Rheumatology.
In patients in which there is clinical suspicion of Takayasu Arteritis,
the erythrocyte sedimentation rate can be superior to 50mm/h,
but only in the early phase.
For a long time,
angiography was the gold standard for the diagnosis.
It allows the diagnosis of stenosis and dilations and has an important role in cases that require intervention with angioplasty or stent placements.
Ultrasonography in the Takayasu Arteritis
Takayasu is an illness that can affect multiple blood vessels,
many of these accessible by US examination.
Their study should be oriented in accordance with the clinical history.
Technique
To evaluate the extracranial primary branches of the aortic arch, linear probes should be used, with ideal frequencies between 10-15 MHz,
with preset of small parts.
The patient should be lying in a supine position,
with the head flat and turned 45º to the side opposite that which is being examined.
The evaluation of the cervical arteries should be initiated in B-mode,
with longitudinal and transversal scans from the clavicle to the mandible,
in such a way to permit an evaluation of the carotid arteries,
carotid bulbes,
internal and external carotid arteries and vertebral arteries. We should pay attention to the the morphology of the arteries,
the presence of fibrocalcified plaques,
and measurement of the intima-media thickness (IMT) of the common carotid artery (CCA) at a distance of at least 5 mm below the distal end of CCA (normal <0.9 mm).
(figure 4)
In the color Doppler and spectral/pulsed waved curves,
with evaluation of the arterial flux and their velocities,
the indications already mentioned in regards to the steering of the color box,
the corrected angle and the filling in by the color of the blood vessel lumen,
remain.
The peak systolic velocity (PSV),
end-diastolic velocity (EDV) and the Internal Carotid Artery / Common Carotid Artery (ICA/CCA) PSV ratio (normal < 2) should be registered.
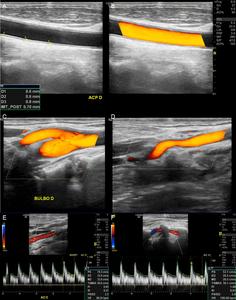
Fig. 4: US B-mode (A) with measurements of IMT on CCA. (B, C, D): Power Doppler demonstrating the CCA, carotid bulbe and External Carotid Artery (ECA) with a kinking. (E, F): Color Doppler with Spectral waves of normal ICA and Vertebral Artery (VA).
Besides the carotid arteries,
US also permits us a good evaluation of the proximal superior limb arteries.
The patient can be lying in a supine position or seated,
with the shoulder girdle relaxed.
The distal portion of the subclavian artery and the axillary arteries should be evaluated through the suprasternal,
supraclavicular and infraclavicular windows.
To evaluate the abdominal blood vessels,
preference should be given to the use of a curved array probe,
with a low frequency.
The patient should be lying in a supine position.
The evaluation should include the supra-renal aorta artery up to the iliac bifurcation,
with longitudinal e transversal scan in B-mode,
where besides identifying atherosclerosis,
is possible to detect aneurysmatic dilations.
In the color Doppler and spectral/pulsed waved curves study,
we can determine the spectral trace and measure the PSV e EDV above the celiac trunk.
The evaluation can be extended to the celiac trunk itself,
superior and inferior mesenteric arteries,
to the renal arteries,
common iliac and external iliac arteries.
At this point,
the imaging quality is just moderate.
The evaluation of the inferior limbs follows the same principles,
it being important to identify stenosis and calculate the PSV at the proximal and distal level in relation to it,
and classify the location,
extension,
and severity.
Expected pathological features
The thickening and parietal edema of the blood vessels are depicted in the ultrasound B-mode as a long segment of diffuse,
homogeneous and circumferential vessel wall thickening.
Contrary to temporal arteritis,
this thickening is midechoic,
with the characteristic Macaroni Sign in the CCA,
which is pathognomonic. (figure 5,
6)
Additionally,
the luminal diameter of the blood vessel can be reduced and the fibrosis can lead to a rigidity increase of the wall,
with analysis by flow and spectral Doppler showing characteristic stenosis or areas of aneurysmal dilation. (figure 5,
6)
Acute occlusions can occur and are identified when hypoechoic material occupies the arterial lumen,
with no evident color signals. (figure 5,
6)
Doppler Ultrasound advantages
Beyond the inherent advantages of the US study itself,
already described,
in this particular case,
US permits differentiating Takayasu Arteritis from GCA due to the Macaroni sign and the absence of the hypoechoic halo.
It also allows adequate evaluation of the carotid,
axillary,
brachial and femoral arteries.
US permits detection of alterations in the pre-stenotic phase and can serve as a screening method when the extracranial and subclavian arteries are evaluated.
US demonstrates benefits comparatively to angiography,
which does not permit an evaluation of the blood vessel wall and is an invasive exam which uses intravenous iodinated contrast and radiation.
MRI or MR-Angiography has been having an increasing role in the diagnosis of TA,
since they allow the visualization of the vessel wall,
as well as measuring the wall edema.
It also permits a quality evaluation of the aorta and its branches,
as well as the determination of the enhancement of the wall,
thus evaluating the state of activity of the illness. (figure 7,
8)
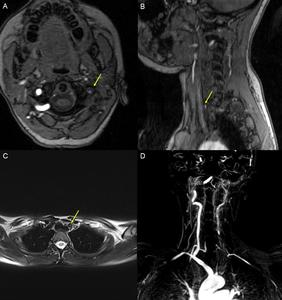
Fig. 7: MR imaging with axial (A ) and sagittal (B) TOF sequences, T2 FS TSE (C) and MIP reconstructions (D) of the patient with Takayasu Arteritis, described in the previous image. It is possible to see, in the left carotid axis, filiform flux in the origin of the CCA (yellow arrows), with the internal carotid diameter significantly reduced and evident irregularities and stenosis. Apparent occlusion of the proximal segment of the left subclavian artery, perfused more distally by a branch with origin in the contralateral subclavian, and apparent occlusion of the primitive carotids and left vertebral artery (D).
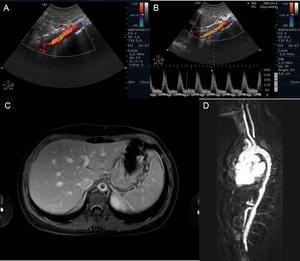
Fig. 8: Color-Doppler and spectral analysis of the flux velocities of a 17 year old female. (A and B) demonstrates, in the segment proximal of the supra-renal abdominal aorta, midechoic parietal thickening with reduction of the permeable lumen and elevated velocities in the order of 300cm/s. MRI axial T1 fat saturation sequences (C) and MIP reconstructions after gadolinium (D) also allow an evaluation of the descending thoracic aorta, which additionally with the supra-renal abdominal aorta, present with reduction of the calibre (10mm) and circumferential parietal thickening with exuberant wall enhancement by the contrast, in relation with active inflammatory alterations .
Computed Tomography (CT),
comparatively to MRI,
can also be used to correctly evaluate the inflammatory alterations of the aorta wall and its branches,
with the particularity of demonstrating the presence of calcifications. (figure 9)
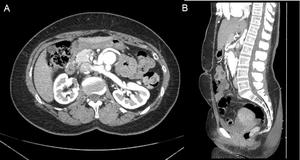
Fig. 9: Axial CT acquisition (A) and reformatted coronal image (B) after iodinated contrast in arterial phase demonstrate occlusion of the native infra-renal abdominal aorta and reconstructed ventral aorta with normal permeability, without stenosis.
However,
both MRI and CT fail in the evaluation of vessels of smaller caliber and the US is superior to the CT or MRI in these arteries,
identifying with assurance,
parietal alterations,
plaques and flux characteristics. (figure 10)
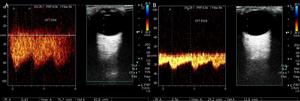
Fig. 10: Color-Doppler and spectral analysis of the flux velocities of the previous patient, with Takayasu Arteritis, demonstrate ophthalmic arteries with normal permeability and weak bilateral spectral profile with ample flux velocities on the right artery ( PSV=75cm/s e EDV=45cm/s) comparatively with the left artery (PVS=30cm/s e EDV=10cm/s).
Doppler Ultrasound limitations
Beyond the limitations of the technique,
already mentioned,
US allows just a moderate evaluation of the proximal subclavian,
iliofemoral,
renal,
superior mesenteric and inferior mesenteric arteries,
of the celiac trunk and the abdominal aorta.
There is no ultrasound access to the thoracic aorta,
with the exception of the transesophageal-ultrasonography.


 and Doppler ultrasound depicting a normal superficial temporal artery, with thin imperceptible and smooth walls and regular lumen, without stenosis.")
 and longitudinal (B) plans, the last one showing a diminished caliber. Color study and power Doppler (C and D) reveal flux turbulence in the region of diminished caliber , due to an increase bigger than twice the velocity in the pre-stenotic segment.")
 and longitudinal (B) plans and also a focal caliber reduction. Color study and power Doppler ( C and D ) reveal flux turbulence in the region of diminished caliber, but without a significant increase of the velocity in the pre-stenotic segment.")
 with measurements of IMT on CCA. (B, C, D): Power Doppler demonstrating the CCA, carotid bulbe and External Carotid Artery (ECA) with a kinking. (E, F): Color Doppler with Spectral waves of normal ICA and Vertebral Artery (VA).")
 and partially obliteration of the arterial lumen (A and B), with weak filling in by color-Doppler effect. (C) Right ICA with flux velocities of low amplitude (D), in an 11 year old patient diagnosed with Takayasu Arteritis.")

 and sagittal (B) TOF sequences, T2 FS TSE (C) and MIP reconstructions (D) of the patient with Takayasu Arteritis, described in the previous image. It is possible to see, in the left carotid axis, filiform flux in the origin of the CCA (yellow arrows), with the internal carotid diameter significantly reduced and evident irregularities and stenosis. Apparent occlusion of the proximal segment of the left subclavian artery, perfused more distally by a branch with origin in the contralateral subclavian, and apparent occlusion of the primitive carotids and left vertebral artery (D).")
 demonstrates, in the segment proximal of the supra-renal abdominal aorta, midechoic parietal thickening with reduction of the permeable lumen and elevated velocities in the order of 300cm/s. MRI axial T1 fat saturation sequences (C) and MIP reconstructions after gadolinium (D) also allow an evaluation of the descending thoracic aorta, which additionally with the supra-renal abdominal aorta, present with reduction of the calibre (10mm) and circumferential parietal thickening with exuberant wall enhancement by the contrast, in relation with active inflammatory alterations .")
 and reformatted coronal image (B) after iodinated contrast in arterial phase demonstrate occlusion of the native infra-renal abdominal aorta and reconstructed ventral aorta with normal permeability, without stenosis.")
 comparatively with the left artery (PVS=30cm/s e EDV=10cm/s).")
