ECR 2018 / C-3135
Single Point of Failure (SPOF) – a useful concept and mnemonic to reduce reporting errors in cancer imaging.
Congress:
ECR 2018
Poster Number:
C-3135
Type:
Educational Exhibit
Keywords:
Education and training, Safety, CT, Oncology
Authors:
S. Junaid1, A. Saeed2, R. White1, G. Joseph1, I. A. Zealley3, A. Yong1, T. Sudarshan3, M. J. Budak3, J. Weir-McCall3; 1Cardiff/UK, 2Swansea, Cardiff/UK, 3Dundee/UK
DOI:
10.1594/ecr2018/C-3135
. The initial report however did not appreciate the enhancing soft tissue component (arrows) in the right lateral aspect of the spinal canal causing malignant spinal cord compression (satisfaction of search). This was later picked up on a subsequent MRI following persistent right arm weakness and the spinal level was treated with radiotherapy. References: NHS")
Fig. 2:
Malignant spinal cord invasion not stated on initial report. This 75-year-old...

Fig. 3:
74-year-old patient with history of localised bladder cancer without metastasis...
 showed a large malignant infiltrating area of abnormal signal in the lower sacrum. Review of MRI (B-T1W) performed 10 months before showed the same lesion to be much smaller and not causing any neural compromise. References: NHS")
Fig. 4:
Patient with history of breast cancer presented with lower back pain and cauda...
 in a staging CT thorax of a 72-year-old male with oesophageal cancer which was not initially appreciated. References: NHS")
Fig. 9:
Pulmonary embolism (arrow) in a staging CT thorax of a 72-year-old male with...
 of the abdominal aorta (just distal to the SMA origin) – a recognised side effect of certain chemotherapeutic agents. The aortic occlusion was initially not reported but later picked up on review of the images. References: NHS")
Fig. 5:
Aortic occlusion not appreciated on initial report. This 58-year-old male was...
 lack of flow void (A - arrow) in the right jugular bulb and ( B-T1 post-contrast) a filling defect (B -arrows) in the right sigmoid sinus and right internal jugular vein consistent with venous sinus thrombosis. References: NHS")
Fig. 7:
Venous sinus thrombosis found on later review of imaging. This 50-year-old...

Fig. 10:
Left external iliac vein thrombosis post chemotherapy. Follow-up scan of a...
. The right portal vein (green ellipse) and main portal vein were normal. Branch portal vein thrombosis is easily missed unless specifically looked for. References: NHS")
Fig. 11:
Left portal vein thrombosis. 28-year-old male patient being treated for...
 and left atrial thrombus (arrows) in a 86-year-old patient with lung malignancy. References: NHS")
Fig. 12:
Splenic vein thrombus (ellipse) and left atrial thrombus (arrows) in a...
 shows an obstructed distal right ureter (arrow) due to an enhancing right pelvic mass, mild hydronephrosis and reduction in perfusion and corticomedullary differentiation of the right kidney. The patient urgently underwent a right nephrostomy and antegrade ureteric stent insertion (B), with nephroureterography demonstrating the malignant stricture (arrow). Review of the initial MRI pelvis 6 months earlier (C, axial T2) demonstrates an abnormal right pelvic nodule (arrow) which was missed at the time and a restaging MRI pelvis at the same level (D, axial T2) shows the nodule has significantly increased in size (arrow). References: NHS")
Fig. 6:
Pelvic nodule causing ureteric obstruction. This 24-year-old patient with a...
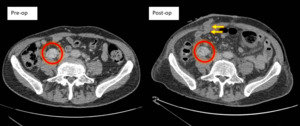
 for a T3 sigmoid carcinoma had a pre-op scan which did not appreciate the metastatic deposit (red circle) adjacent to the right ureter which may be an abnormal node or peritoneal disease. The post operative CT was done to look for an anastomotic leak. This patient would have likley presented in the near future with right ureteric obstruction. References: NHS")
Fig. 13:
Metastatic deposit adjacent to the right ureter. This 80-year-old patient had...

Fig. 14:
Sub-total obstruction with left colon cancer. Long segment of concentric left...
 showed a type B dissection. A subsequent CT (C) showed left upper lobe segmental collapse (yellow arrows) secondary to an endobronchial lesion which was also present on the initial scan (B - red arrow). Histologically this was carconoid. References: NHS")
Fig. 16:
Endobronchial nodule which subsequently caused segmental collapse. 58-year-old...
 showed that the third part of the duodenum (red arrows) was obstructed between the Aorta (Ao) and the SMA (yellow arrow). In our experience, patients with sudden weight loss secondary to cancer can lose some retroperitoneal fat around the duodenum and in certain cases increase the risk of developing SMA syndrome. References: NHS")
Fig. 17:
SMA syndrome causing duodenal obstruction. This 58-year-old patient with...
 showed a large lytic lesion in the right proximal femur which is at high risk of fracture (A-arrow). CT of the abdomen and pelvis (B - coronal) and ( C- axial) performed four months earlier reported no recurrent malignancy, however, a small lytic lesion in the right proximal femur was present at that time (B and C arrow). The patient was subsequently managed with surgical nailing of the right femur. References: NHS")
Fig. 8:
Proximal femur metastasis at risk of fracture. This 60-year-old with a history...
 following minimal trauma. Review of previous chest radiograph (A) performed 4 months earlier showed subtle cortical destruction (red arrows) which was not seen at the time. References: NHS")
Fig. 18:
Right proximal humeral metastasis which subsequently fractured. Patient with...

Fig. 19:
Left main bronchus lesion not appreciated on initial report. The coronal CT...

Fig. 1:
Single Point of Failure