In this exhibit we provide an illustrated summary of US findings of typical and atypical,
confusing patterns of focal fatty liver and its clinical implications.
Patrick- Olivier Decarie et al [4] identified six patterns of liver steatosis:
diffuse- most prevalent, geographic, focal,
subcapsular,
multifocal and perivascular
Common patterns of hepatic steatosis include:
- diffuse fat accumulation
- diffuse fat accumulation with focal sparing
- focal fat accumulation in an otherwise normal liver.
The typical manifestations of focal fatty sparing are:
a geographic configuration,
a poorly delineated margin, no space-occupying effect, no displacement of adjacent vessels,
and similar contrast enhancement compared with the normal liver parenchyma
Its most common shape resembles a spot,
band or ring [5].
Diffuse fatty liver with focal sparing is located characteristically in specific areas.
They usually occur:
- in the posterior edges of segments II and IV,
- in the medial segment of the liver along the gallbladder fossa
- the posterior edge of segment IV (aberrant left gastric vein).
However,
it can occur in other parts of the liver and show a heterogeneous or nonuniform distribution of fat,
that can mimic malignancies.
Atypical cases of FFS are known to pose a diagnostic challenge especially in an oncological setting,
especially in cancers with higher propensity for liver metastases.
Such atypical patterns include:
- Perivascular FFS- dif.dg.: periportal oedema,
passive hepatic congestion and Budd–Chiari syndrome (CT and US- MRI)
- Multifocal nodular fatty infiltration of the liver (MNFIL) mimicking metastases
- Single or multiple mass-like FFS in atypical liver segments,
with atypical appearence- wedge shaped FFS- peritumoral sparing- cases of metastatic liver tumor masquerading as a wedge- shaped area of focal sparing in a fatty liver- result of diminished blood flow from the vascular compression or nodular- mimicking meteastasis
Conversely,
some cases of true hepatic masses have been reported to mimic fatty infiltration or focal sparing.
Common patterns of FFS:
-A 60 year-old patient with history of DM,
AH,
no history of of other hepatic disease,
no alcohol consumption- his routine annual abdominal ultrasonographic examination,
performed by different sonologist,
showed a common pattern of FFS- a hypoechoic geographically configured area with poorly delineated margins in segment IV with moderate background hepatic steatosis.

Fig. 3: Transabdominal US in B-mode examination shows in liver segment IV a hypoechoic geographically configured lesion (between crosses) with poorly delineated margins, and with no space-occupying effect. The maximal diameter of the lesion is 5.07 cm.
Typical FFS- transabdominal US in B-mode examination shows in liver segment (between crosses) with poorly delineated margins,
and with no space-occupying effect.
The maximal diameter of the lesion is 5.07 cm.

Fig. 4: Typical FFS- Color Doppler image showing no vascular displacement.
Typical FFS- Color Doppler image showing no vascular displacement.
Characteric US features of typical FFS:
- typical shape
- typical location
- no mass effect
- stability in size
- intralesional vascularisation
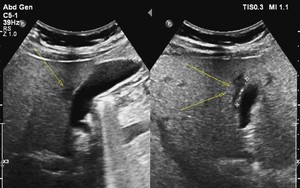
Fig. 1: Sonogram shows a polygon-shaped hypoechoic area (arrows) adjacent to the gallbladder bed of the liver.
A typical FFS- a polygon-shaped hypoechoic area (arrows) adjacent to the gallbladder bed of the liver.
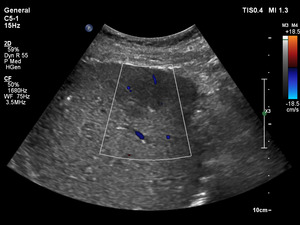
Fig. 18: Color doppler shows intralesional vascularization- a typical US feature of FFS.
Subcapsular FFFS with intralesional vascularization.
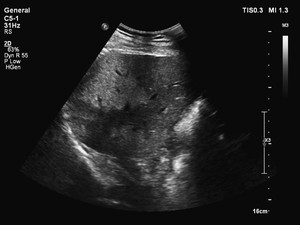
Fig. 2: Sonogram shows a segmental fatty steatosis and focal sparing causing an inhomogeneous liver. (transabdominal US scan, convex probe, 5 MHz).
Sonogram shows a segmental fatty steatosis and focal sparing causing an inhomogeneous liver.
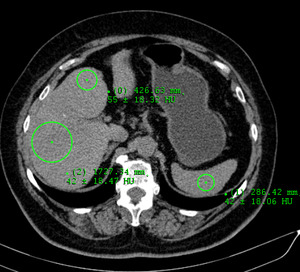
Fig. 17: Axial unenhanced CT scan shows normal liver parenchyma- average attenuation of liver parenchyma on non-contrast CT images varies between 50 and 65 HU and is generally 8-10 HU greater than that of spleen.
Axial CT scan- geograogic pattern of hepatic steatosis.
- Typical band-like FFS in patient with history of malignancy
A 77 year-old female patient with history of breast cancer (2012.) and recurrent ovary carcinoma (2015),
NAFLD with moderately altered liver enzymes; she was treated with mastectomy,
hysterectomy,
adnexectomy,
chemotherapy,
radiotherapy,
and adjuvant chemotherapy consisting of trastuzumab. For the last year she is taking tamoxifen, which is associated with the development of NAFLD and NASH (non alcoholic steatohepatitis).
[6]
Her routine annual abdominal ultrasound examination showed in liver segment V a hypoechoic band-like shaped area,
and one hypoechoic area with a wedge shaped in liver segment VII.
Both lesions showed no mass effect,
and normal vascularization was detected using a color Doppler ultrasound examination.
These are typical areas of FFS.
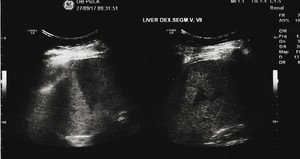
Fig. 5: Transabdominal US in B-mode examination shows in liver segments V and VII hypoechoic areas with band-like and triangular shape, with no vascular displacement, in background fatty liver.
Transabdominal US in B-mode examination shows in liver segments V and VII hypoechoic areas with band-like and triangular shape,
with no vascular displacement.
Axial unenhanced CT scan from 2010,
show normal liver parenchyma.
(Average attenuation of liver parenchyma on non-contrast CT images varies between 50 and 65 HU and is generally 8-10 HU greater than that of spleen. [7]
KEY POINTS:
- If previous radiologic finding showed homogeneous fatty liver,
then new focal abnormality on a follow-up sonography would require further workup,
and other focal lesions should be considered,
such as metastatic liver tumor masquerading as a wedge-shaped area of FFS in fatty liver.
Atypical patterns of FFS:
-A 65-year old man with a history of 17-year insulin-trated type 2 diabetes mellitus,
obesity and dyslipidemia,
a 10- year history of arterial hypertension and new clinical onset of microcytic anemia normal liver laboratory tests- new FFS was found in previously diffuse homogeneous fatty liver.
A round nodular hypoechoic area with well- defined margin and presence of space-occupying effect was determined at his routine annual abdominal ultrasound examination in liver segment IV.
The diameter of the lesion is 9 mm.
The area shoed no posterior acoustic attenuation.
Absence of vascularity was detected on color Doppler flow and power Doppler imaging.

Fig. 6: Sonogram of a patient hospitalized because of uncontrolled insulin-dependent DM (diagnosed in 2000.) and microcytic anemia shows a nodular pattern in previously diffuse homogenous fatty liver- true lesion?
Sonogram of a patient hospitalized because of uncontrolled insulin-dependent DM (diagnosed in 2000.) and microcytic anemia shows a nodular pattern in previously diffuse homogenous fatty liver- true lesion?
Since in our institution MRI is not still implemented,
the patient underwent MRI in an other institution,
since he refused liver biopsy.
KEY POINTS:
-Previous sonographic findings of the liver may be used for reference when a tumorlike abnormality is found on follow-up sonography
- If previous radiologic finding showed homogeneous fatty liver,
then new focal abnormality on a follow-up sonography would require further workup,
and other focal lesions should be considered. [8]
-A 68 year-old with history of colon cancer,
anemia and NAFLD -
His regular US examination showed one irregulary shaped,
hypoechoic areas with poor-lined margins,
which size was 14-17 mm in both of liver lobes.
His previously sonography is used for reference- showed diffuse homogeneous fatty liver,
so these new focal abnormalities requested further work-up.

Fig. 24: US examination showed an irregulary shaped, hypoechoic areas with poor-lined margins, which size was 14-17 mm in each liver lobe.
The patient underwent CT scanning,
which revelead an irregular,
heterogeneous lesion,
which maximal diameter was 18x 9 x 13.2 cm.
On unenhanced CT scan the lesion showed enhancement (20 HU),
in the arterial phase 50-60 HU and in the portal phase 80 HU.
In the delayes phase no wash-out effect was shown.
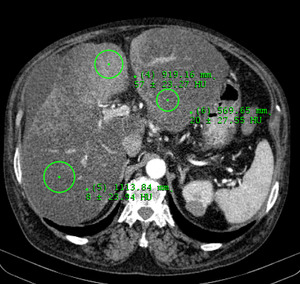
Fig. 19: During the arterial phase the liver lesion shows enhancement.
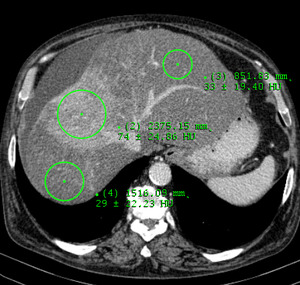
Fig. 20: Portal venous phase. Intact vascular supply.
In the affected area,
no vessel displacement was detemined.

Fig. 21: 3D CT reconstruction showing intact vascular supply in the affected area.
Biopsy of the lesion was performed.
Anatomopathological examination showed micro and macrovesicular steatosis with lymphocityc infiltration.
Niether fibrosis nor tumor cells were present.
Serological examination showed chronic hepatitis B infection.
Liver tests were not altered.
Criteria for HCC were excluded,
so MRI was reccomended.
-FLL with peritumoral sparing in patients with hepatic steatosis= atypical sonographic appearance.
-The focal fatty sparing can obscure the presence of FLL or at least modify the sonographic appearance,
leading to diagnostic confusion.
[9]
- Peritumoral focal sparing can be the only clue for space occupying lesion in the liver- often fan- or wedge-shaped.
Etiology:
Focal peritumoral sparing may result from regionally decreased portal flow,
caused by a space-occupying lesion through several mechanisms:
- less fat or toxins (e.g..
alcohol or chemotherapeutic drugs) coming from the portal vein are delivered to the hepatocytes in regions of decreased portal flow;
- · only hepatocytes that are metabolically normal are susceptible to fat deposition [10]
- · and because deprivation of portal flow inhibits the function of hepatocytes,it also prevents fat deposition.
A more important type of focal sparing caused by a tumor and located around it may appear as a hyperattenuating thin ring or a thick irregularly shaped rim (width,
2-20 mm), surrounding a hypoattenuating tumor on unenhanced CT images.
[11]
-When there is no attenuation difference between the tumor and the focal sparing on unenhanced and/or enhanced CT,
the tumor may mimic ordinary (non-tumor-related) focal sparing of the fatty liver induced by normal variants of the portal venous system.
-Thus,
the tumor associated with peritumoral sparing appears as a round or irregular hyperattenuating mass in the fatty liver.
It may disguise itself as ordinary focal sparing when an irregularly shaped homogeneous mass is located in the subcapsular region.
The cause of peritumoral sparing is also explained by the absence of portal blood flow to this area [12].
This finding is important since it can be the only finding in some cases,
indicating the existence of a mass.
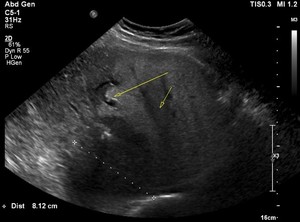
Fig. 16: Atypical FFS pattern with FLL- peritumoral sparing of fatty infiltration is present around metastatic lesion.
70 years old with hepatic steatosis and metastasis from CRC.
Peritumoral sparing of fatty infiltration is present around metastatic lesion.

Fig. 22: Unenhanced axial CT scan demonstrates inhomogeneous fatty liver with FLL.
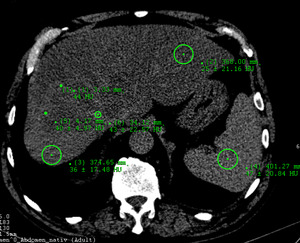
Fig. 23: Unenhanced CT axial scan- the presence of a hyperattenuating rim around the nodule helps distinguish the lesion from ordinary FFS.
On CT,
the presence of a hyperattenuating rim around the nodule helps distinguish the lesion from ordinary FFS.
- However,
when radiologists are faced with a wedge- shaped rather than a spheric or ovoid liver lesion (which may simulate a tumor on sonography or CT,
so there is a high index of suspicion when radiologists find a spheric or ovoid liver lesion) the risk of overlooking a malignant tumor increases.
KEY POINTS:
-Most of the time,
focal sparing is a benign condition,
however,
occasionally,
it is caused by a malignant tumor.
-Asses wedge- shaped focal sparing carefully- rule out the possibility of a tumor near the radix of the focal sparing
-When round or irregularly shaped focal sparing is encountered in the fatty liver,
a tumor with or without peritumoral sparing should be ruled out. [13]
-It is important for radiologists both to recognize peritumoral sparing so that it can be identified as a sign of adjacent focal lesions.
- Multinodular FFS and perivascular fat sparing
A 43 year-old man with no history of systemic disease nor malignancy.
He does not consume alcohol,
no history of smoking.
Clinical examination revealed no abnormality.
Laboratory results,
including hepatic tests were normal.
He reports a daily diet in fat content.
His regular ultrasound examination (6/2017) showed diffuse homogeneous fatty liver with four hypoechoic hepatic nodules,
the size 8-13 mm in liver segment VI of uknown origin.
They were well-delineated,
homogeneous,
without mass effect.

Fig. 7: Sonogram shows diffuse homogeneous fatty liver with four hypoechoic hepatic nodules, the size 8-13 mm in liver segment VI of uknown origin. They were well-delineated, homogeneous, without mass effect.

Fig. 8: Sonogram shows multifocal well-delineated hypoehogenic nodules.No posterior acoustic attenuation.
A 6-month follow-up ultrasound examination was recomended,
which reveled progression in number and size of FLL,
the maximal diameter measured was 1.7 cm.
General examination findings were still unremarkable.
In addition,
perivascular hipoechoic areas,
with no vessel displacement were determined.
It may be difficult to differentiate perivascular fat deposition or perivascular sparing from periportal oedema,
passive hepatic congestion and Budd–Chiari syndrome on CT and ultrasound.
MRI is useful for making this rare diagnosis by showing a signal intensity loss on opposed-phase images compared with in-phase images.
The pathogenesis of perivascular fat sparing is unknown.
[14]
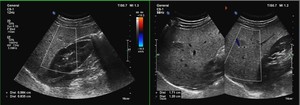
Fig. 9: Follow-up sonogram shows progression in size of the hypoehogenic nodules with no vascular displacement.
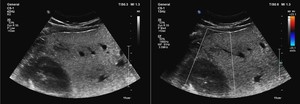
Fig. 10: Follow-up sonogram shows progression in number and size of the hypoehogenic nodules. Perivascular fat sparing is also detected.
To exclude a suspicion of cavernous hemangiomas,
the same day he underwent a CT examination.
CT scanning in hepatic arterial,
portal venous,
and delayed phases was performed.
Unenhanced CT scans demonstrate well- delineated oval shaped lesions in liver segments III,
IV,
VII and VIII,
which size ranges from 13 to 23 mm,
with no mass effect,
enhances in all phases after injection,
without wash-out during the late phase.
No other lesion was found.
The hepatic nodules corresponded to fatty sparing areas- the diagnosis of multinodular fatty sparing was determined.
The diagnosis of fatty sparing in areas of multinodular appearance is diffucult.
-The differential diagnosis on CT and ultrasound may include metastasis,
lymphoma,
sarcoidosis,
abscesses,
candidiasis,
haemangiomatosis and biliary hamartomas,
regenerative nodules in severe alcoholic toxic cirrhosis.
MRI is usually required to make the diagnosis.
-In a seriously ill patient who is in poor general condition and has a history of cancer and/or abnormal blood test results,
the diagnosis of malignant disease (usually metastatic) is obviously most likely; on the contrary,
in young,
fit and asymptomatic patients who have normal blood test results and no relevant past medical history,
other possible diagnosis must be considered.
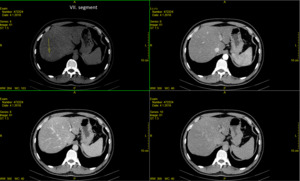
Fig. 11: Technique of choice- unenhanced axial CT, arterial, portal venous and delayed imaging phase. The unenhanced CT axial scan shows well- delineated oval shaped lesions with no mass effect.
In the arterial, portal venous and delayed imaging phase there is typical enhancement after contrast injection -that parallels the background liver parenchyma.
No wash-out effect during the delayed phase.
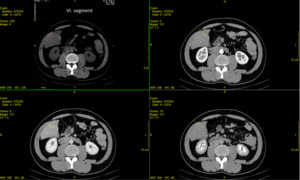
Fig. 12: Technique of choice- unenhanced axial CT, arterial, portal venous and delayed imaging phase- show typical features for FFS- liver segment VI.
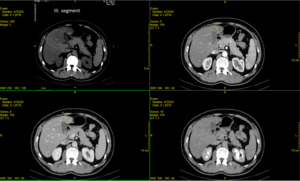
Fig. 13: Technique of choice- unenhanced axial CT, arterial, portal venous and delayed imaging phase- show typical features for FFS- liver segment III.
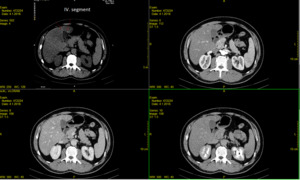
Fig. 14: Technique of choice- unenhanced axial CT, arterial, portal venous and delayed imaging phase- show typical features for FFS- liver segment IV.
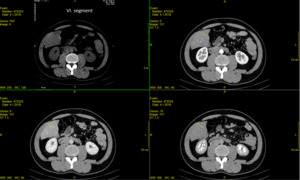
Fig. 15: Technique of choice- unenhanced axial CT, arterial, portal venous and delayed imaging phase- show typical features for FFS- liver segment VI.
