ECR 2018 / C-3214
Update on Imaging of Pulmonary Venous and Arterial Tumors
Congress:
ECR 2018
Poster Number:
C-3214
Type:
Educational Exhibit
Keywords:
Pulmonary vessels, Oncology, Lung, CT, CT-Angiography, Diagnostic procedure, Education, Staging, Cancer, Embolism / Thrombosis, Neoplasia
Authors:
A. Mehta1, P. Rajiah1, M. Landay2, S. Abbara1, K. Jordan2, A. Kandathil2, S. Saboo2; 1Dallas, TX/US, 2Dallas/US
DOI:
10.1594/ecr2018/C-3214
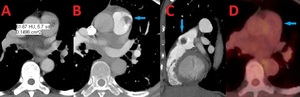
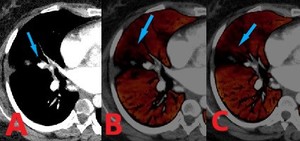
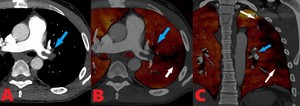
. Contrast enhanced computed tomography (CT) axial image shows a hypodense 1.4 x 1 cm pulmonary arterial mass. (C). Contrast enhanced computed tomography (CT) sagittal image shows this hypodense lesion just distal to the pulmonic valve. (D). Axial image from FDG PET scan shows that the pulmonary artery mass is not significantly FDG avid.")
Fig. 1:
67 yo F with a pulmonary artery mass found to be a benign papillary...
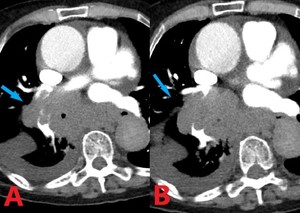
. (A). Axial image shows a 3.6cm transverse x 2.4 cm anteroposterior x 4 cm craniocaudad mass involving the right superior pulmonary vein and left atrium. (B). Axial image at a slightly lower level shows further extension of filling defect involving the right superior pulmonary vein (blue arrows).")
Fig. 2:
39 yo F with spindle cell sarcoma of the right superior pulmonary vein and left...
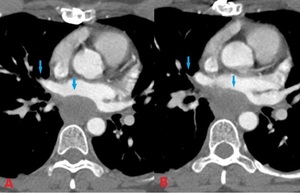
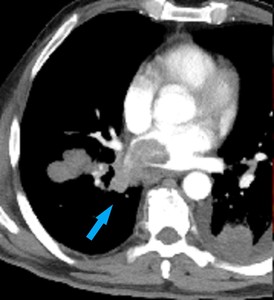
. (A). Axial image demonstrates local invasion into the right lower lobe branch pulmonary artery (blue arrow). (B). Axial image at slightly lower level shows encasement and invasion into the branching pulmonary artery by the primary tumor.")
Fig. 3:
71 yo F with metastatic small cell lung cancer and invasion into right lower...
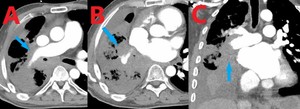
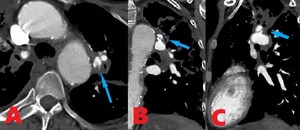
. (A) Axial image demonstrates encasement and invasion of the right pulmonary artery. (B) Axial image at a slightly lower level shows further involvement of the right pulmonary artery branches. (C). Coronal image reveals local spread of primary adenocarcinoma into the right pulmonary arterial vasculature.")
Fig. 4:
61 yo M with primary adenocarcinoma of the lung with invasion of the right...
 Coronal contrast enhanced CT image and (B) Coronal MIP from PET scan showing pulmonary venous extension of a LUL lung mass. Histopathology confirmed high grade sarcomatoid (spindle cell) carcinoma with necrosis and invasion into the pulmonary venous vasculature.")
Fig. 5:
66 yo M with recent diagnosis of LUL mass, previously treated for pneumonia....
. Axial CT soft tissue window of the mid-lower lung shows cutoff of the lateral segmental bronchus of the right middle lobe and adjacent lateral subsegmental pulmonary artery branch from osteosarcoma metastasis (arrow) along with mucous/debris. (B and C). Corresponding section lung perfusion images from dual energy CT data reveal right middle lobe lateral subsegmental parenchymal perfusion defect (arrows).")
Fig. 6:
32 yo F with chest pain in patient with metastatic osteosarcoma. (A). Axial CT...
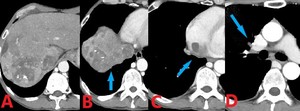
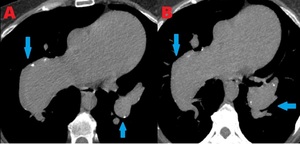
. (A-B). Axial images through the liver demonstrate a heterogeneously enhancing mass, consistent with known hepatocellular carcinoma. (C). Axial image reveals tumor invading the IVC at the junction of the right atrium. (D). Axial image shows a filling defect in the right pulmonary artery, representing a tumor embolus.")
Fig. 7:
52 year old male with metastatic hepatocellular carcinoma invading the IVC and...
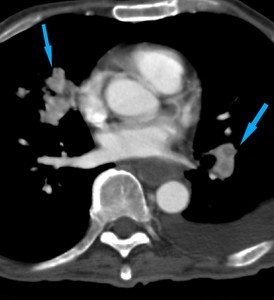
 image shows nodular heterogenoulsy enhancing serpiginous opacities within the bilateral pulmonary arterial vasculature consistent with endovascular RCC tumor emboli.")
Fig. 8:
63 year old male with metastatic renal cell carcinoma. Contrast enhanced axial...
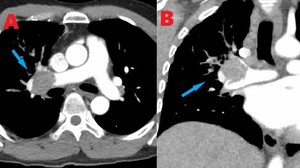
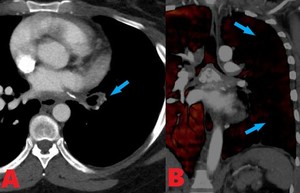
. (A). Axial image shows tumor emboli in the distal right pulmonary artery. (B). Coronal image further demonstrates this finding with a filling defect seen in the right pulmonary artery.")
Fig. 9:
67 yo M with metastatic renal cell carcinoma and tumor emboli in the right...
. Contrast enhanced axial computed tomography (CT) image shows tumor emboli in the left pulmonary artery. (B). Lung perfusion axial image acquired from Dual Energy scanner shows tumor emboli in the left pulmonary artery (blue arrow) and peripheral perfusion defect (white arrow). (C). Lung perfusion coronal image shows tumor embolus (blue arrow) and extensive peripheral perfusion defect (white arrows).")
Fig. 10:
35 yo M with metastatic renal cell carcinoma with tumor emboli to the left...
 image demonstrates a filling defect and spread in the right inferior pulmonary vein (arrow).")
Fig. 11:
57 year old male with metastatic melanoma infiltrating right inferior pulmonary...
. Contrast enhanced computed tomography (CT) axial image shows a homogenous hypodense filling defect spanning the bifurcation of the pulmonary artery consistent with a saddle embolus. (B). Contrast enhanced computed tomography (CT) axial image shows thrombotic emboli into the branching pulmonary arteries. (C). Contrast enhanced computed tomography (CT) coronal image demonstrates hypodense emboli in the right and left pulmonary arteries (arrows). (D). Coronal lung perfusion image shows areas of decreased perfusion secondary to pulmonary emboli.")
Fig. 12:
83 yo F with extensive bilateral pulmonary emboli including a saddle embolus....
. (A-B). Axial MIP and soft tissue window images reveal marked dilated main, right and left central pulmonary arteries secondary to eccentric chronic thrombus in right pulmonary artery. Patchy bilateral pulmonary artery wall calcifications are seen due to pulmonary artery hypertension.")
Fig. 13:
55 yo M with dilated pulmonary arteries secondary to chronic emboli. Contrast...
. Contrast enhanced computed tomography (CT) axial image shows marked attenuation of the left lower lobe pulmonary arteries. (B). Lung perfusion coronal image shows perfusion defects in the peripheral left lung (blue arrows), secondary to fibrosing mediastinitis.")
Fig. 14:
39 yo F with fibrosing mediastinitis. (A). Contrast enhanced computed...
. Axial image shows a pseudoaneurysm arising from the superior margin of the left main pulmonary artery sitting adjacent and medial to the apicoposterior pulmonary arteries feeding the left upper lobe. (B-C). Coronal images showing a pseudoaneurysm of the left main pulmonary artery.")
Fig. 15:
54 yo M with a pseudoaneurysm of the left main pulmonary artery. Contrast...
. (A) Axial and (B) coronal images show filling defects and abrupt cut off of the left main pulmonary artery without opacification distally secondary to mucormycosis.")
Fig. 16:
30 yo F with invasive rhizopus infection. Contrast enhanced computed tomography...
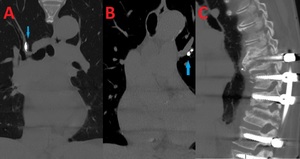
 images. (A-B). Coronal images show hyperdense lesions in the right (A) and left (B) branching pulmonary arteries representing embolized cement. (C). Sagittal image shows evidence of prior spinal surgery.")
Fig. 17:
77 yo F with cement pulmonary emboli secondary to multiple prior surgeries...

Table 1