-after a close review of the specialty literature,
some of the issues found need to be mentioned:
- the nomenclature: in the past,
regardless of their nature and histopathological mechanism,
all HIV related salivary gland lesions containing cysts were considered altogether as being ARPC (AIDS-related parotid cysts)5. This term can cause confusion because it doesn’t specify which type of HIV-SGD (BLEC,
BLEL or another salivary lesion which later developed cysts) refers to,
and by considering two or more pathologies as being the same one it can lead to mistreatment,
as the therapeutic approach and general management of each one is different. Fig. 2
- BLEC vs.
BLEL- many if not most authors consider these two lesions as being one and the same.
Although they have some common aspects,
the overall methodology,
evolution,
and management are different6;
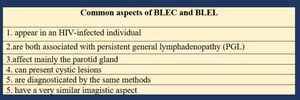
Fig. 3: Comparison between BLEC and BLEL - common aspects
References: Dr. Paul-Andrei Stefan, "Iuliu Hațieganu" University of Medicine and Pharmacy, Cluj-Napoca, Romania
- while BLEC is defined as single or multiple cysts within lymph nodes situated mainly along the tail of the parotid gland that have been trapped during parotid gland embryogenesis,
BLEL may arise separately from an auto-immune mediated response.
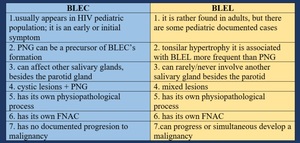
Fig. 4: Comparison between BLEC and BLEL - the most important differences
References: Dr. Paul-Andrei Stefan, "Iuliu Hațieganu" University of Medicine and Pharmacy, Cluj-Napoca, Romania
GENERAL PRESENTATION

Fig. 5: General presentation
References: Dr. Paul-Andrei Stefan, "Iuliu Hațieganu" University of Medicine and Pharmacy, Cluj-Napoca, Romania
DIAGNOSIS OF HIV-SGB
step 1: Clinical Assesment - should accurately determine the following:
- a sudden increase in gland size should arouse suspicion of possible lymphomatous transformation7;
-some features of malignant transformation include induration,
pain,
fixation,
and facial nerve pathology.
step 2: Imaging diagnosis
2.1 General features8
- although ultrasound and MRI are considered to be the best options in the imaging evaluation of the salivary gland disease,
there are some authors that consider that in the case of a patient who is known to suffer from an HIV infection and also presents salivary gland enlargement,
the Contrast-Enhanced CT (CECT) will be the correct first choice in investigating this disorder;
- CECT may be considered the best imaging tool because it can characterize more accurately the cystic walls,
tonsilar hyperplasia,
solid parotid masses,
and the cervical lymphadenopathy;
- it is generally considered that if the ultrasound and FNAC are conclusive there should be no further imaging evaluation.
However,
there are some authors that consider the CECT the first image modality to evaluate the cystic lesions if BLEC is suspected.
Since BLEC only manifests through cysts and lymphadenopathy,
it is quite difficult to rule out solid lesions and tonsillar lymphadenopathy just by ultrasound,
therefore the CECT will be a recommended choice9.
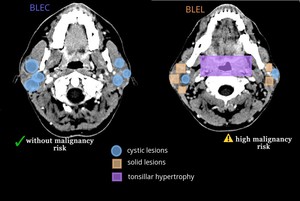
Fig. 6: The hypothetical differences between BLEC and BLEL observed in a contrast-enhanced CT scan. The risk of malignancy is also mentioned.
References: Department of Radiology, Hospital of Infectious Diseases, Cluj-Napoca
2.2 Ultrasound
- ultrasonography allows for evaluation of both cystic and lymphoproliferative lesions of the parotid glands8;
- In children,
ultrasound may be preferred because it is less invasive and does not require sedation or radiation exposure;
- four distinctive ultrasound patterns of HIV-SGB affecting the parotid gland have been established: Fig. 7
1) lymphocytic aggregations (= solid intraparotid lesions) – may be suggestive for BLEC; usually appear heterogeneous and measure less than 5 cm,
this aspect can be suggestive for an intraparotid lymphadenopathy.
2) lymphoepithelial cysts – appear as round hypo-echoic areas with well-circumscribed margins and internal septa;
3) fatty infiltration (in cases of patients treated with protease inhibitor medication).
4) lymphadenopathy – in the cervical region; it doesn’t involve necrosis.
2.3 FNAC (Fine needle aspiration cytology)
- FNAC it is generally ineffective for BLEC’s treatment because the cysts recur in weeks,
but it may be the most valuable diagnostic tool;
- recommendations for FNAC in case of BLEC of the adult HIV-infected population:
1.
always when there are 2 or fewer cysts (imaging diagnosis unclear);
2.
sometimes when there are 3 or more cysts (even in this case the imaging diagnosis clear) to rule out other pathology (exclude the lesions that may be considered in the differential diagnosis).
- recommendations in case of BLEL of the adult HIV-infected population: FNAC is is indicated in all cases.
- In children,
these recommendations may not be as strictly enforced because FNA is not always well tolerated by this age group.
- common FNAC findings6:
|
BLEC
|
BLEL
|
|
- yellow mucous type fluid
- heterogeneous lymphoid population
- scattered foamy macrophages
- anucleated squamous cells
- proteinaceous background
|
-Immunoblasts
-active phagocytosis of nuclear
debris
- lymphoid aggregates
- myoepithelial islands
|
2.4 CT
- as it was mentioned before,
the CT scan may be one of the most important diagnostic imaging tools
- the aspects found in the CT scan are not pathognomonic but can be highly suggestive for HIV-SGD.
It is very important to administer contrast in order to differentiate solid lesions from the rest of the normal parenchyma of the parotid gland. Fig. 8
- the main aspects of HIV-SGD (BLEC and BLEL) revealed by both native and contrast-enhanced CT scan are as follow:
2.4.1 non-enhanced CT-scan (NECT) can disclose both the parotid cysts,
usually appearing well-circumscribed and the solid masses,
the last one with smaller accuracy.
Also,
the parotid glands appear enlarged.
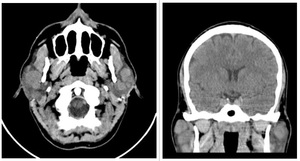
Fig. 9: Axial and coronal native CT scan of a 30 y.o. patient with HIV-infection shows bilateral parotid enlargement and cysts, but no tonsillar hypertrophy or solid lesions which suggests that BLEC is the more accurate diagnosis.
References: Department of Radiology, Hospital of Infectious Diseases, Cluj-Napoca
2.4.2 Contrast-enhanced CT-scan (CECT) show also the parotid gland enlargement,
this time showing hyperdense.
The cystic lesions appear to have a thin rim enhancement.
In the case of BLEL,
the solid lesions show heterogeneous enhancement and the tonsilar hypertrophy is visible.
Fig.
10
- the solid lesions of BLEL are best characterized by observing their behavior before and after the contrast.
While on the native examination they appear as hetero-dense lesions,
they enhance after the admission of the contrast substance Fig. 10
2.5 MRI
- in general,
the MRI scan supports the CT findings;
On T1WI,
the cystic lesions have low signal,
and the solid lesions have a heterogeneous signal.
On T2WI,
both the cervical lymphadenopathy and the lymphatic ring appear hyperintense.
The cysts appear as hyperintense and well-circumscribed ovoid intraparotid masses.
On T1WI with contrast,
cystic lesions have a thin rim enhancement,
but this particular sequence it's not so good for characterizing the solid lesions because of the surrounding fat.
Differential diagnosis:
-when BLEC manifests itself as a unilateral cystic mass in the parotid it can be mistaken for the first branchial cleft cyst
- when BLEL manifests initially as a unilateral solid intraparotid mass it may be mistaken for a parotid tumoral process
- Warthin tumor
- Sjogren syndrome
- Sarcoidosis involving the parotid gland
MANAGEMENT
Several common aspects of the management of HIV Parotid Lesions:
- observation - in asymptomatic patients and most children
- aspiration - it is generally ineffective because cysts recur within weeks
- low-dose external radiation therapy and antiretroviral medication can be considered
-
the follow-up and treatment protocol (especially surgical) of the two lesions (BLEC and BLEL) are different,
as well as the long-term implications,
and they are all based on the correct diagnosis of the lesion.



 Diagnostic ultrasound patterns of parotid glands in human immunodeficiency virus-positive patients in Mulago, Uganda")



. References: Department of Radiology, Hospital of Infectious Diseases, Cluj-Napoca")