
Table 1: Table of contents
BIRADS classification is the standard for breast imaging reporting.
Different terms have been employed for asymmetric findings on mammography in different BIRADS editions.
-1st ed (1993) / 2nd ed (1996)/ 3rd ed (1998).
Terms included were:
Density .
A noncalcified finding seen only on one of the two standard mammographic views
Focal asymmetric density .
A non-mass finding seen on at least two views that occupies less than a quadrant.
Asymmetric breast tissue. A non-mass finding seen on at least two views that occupies at least a quadrant.
-4th ed (2003).
The term Asymmetry appeared,
employed in place of density.
• Asymmetric tubular structure/dilated duct,
• Focal asymmetry
• Global asymmetry
-5th ed (2013).
Asymmetries are now described as an independent section,
and the new term Developing asymmetry appears.
The new Section (D) describes Asymmetries,
including:
| • Asymmetry |
| • Focal asymmetry |
| • Global asymmetry |
| • Developing asymmetry |
| 2.
BIRADS Fifth edition classification and definition of asymmetries on mammograms: |
The definition of asymmetries included in the last edition (5th) of BIRADS consists of:
• Asymmetry.
Unilateral area of fibroglandular tissue density visible on only one mammographic projection.
• Global asymmetry.
Large area of at least one quadrant of fibroglandular density greater than the same area in contralateral breast. It is seen on two projections,
but has concave outwards borders and is interspersed with fat.
• Focal asymmetry.
Small area of less than one quadrant of a greater fibroglandular tissue density compared to contralateral breast.
It is seen on two projections,
with concave outwards borders and is interspersed with fat. It has similar shape on two views but does not fit the criteria of a mass (lacks outer border.
• Developing asymmetry.
A focal asymmetry which is new,
larger or more conspicuous than on previous studies.
| 3. Different causes of asymmetries ( Fig. 1 ). |
Breast asymmetries may have different causes either benign or malignant.
The different entities included in differential diagnosis are:
Benign.
• Summation artifact.
• Normal variant
• Asymmetrical breast tissue
• Hormonal changes
• Fibrocystic changes
• Pseudoangiomatous stromal hyperplasia (PASH)
• Inflammatory.
• Diabetic mastopathy
• Granulomatous mastitis
• Fat necrosis,
hematoma
Malignant
• Invasive ductal or lobular carcinoma
• DCIS
• Lymphoma (rare).
Fig. 1: Causes of Breast asymmetries.
| 4. Diagnostic work-up of asymmetries ( Fig. 2 ). |
Due to the possibility that an asymmetry may be malignant and the overlapping in imaging from different causes,
a systematic diagnostic work-up is essential in the evaluation of breast asymmetric findings.
The steps for imaging evaluation would be as follows:

Fig. 2: Asymmetric findings. Diagnostic work-up.
4.1.Confirm the image is real and whether it appears in one or two projections.
First it is important to be sure that an image is real,
not caused by summation artifact.
Furthermore when the image is clearly seen on mammograms in one projection it should be investigated whether it is also apparent on other projections,
which would determine the type of asymmetry.
4.1.1.Correct technique.
In order to find out whether an asymmetric finding on mammogram is a real lesion the first step in evaluation is to confirm that mammography technique is adequate.
• Position.
Signs of proper positioning should be analyzed,
as the area may have not been represented in one view ( Fig. 3 ).
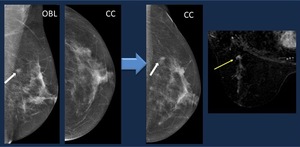
Fig. 3: Correct technique: Mammogram. An asymmetry detected on oblique view (arrow) is not visible on CC view. A forced CC view depicts the lesion (arrow). MR confirms the enhancing nodule. Core biopsy. Infiltrating ductal carcinoma
• Compression. Undercompression of breast may be causing an spurious image.
4.1.2.
Expected lesion location.
When a lesion is depicted on one view you should look for it on the second projection.
Knowledge of the expected location helps to find it.
• Distance: Arch method.
When you measure the distance from the nipple to the lesion seen on one view, you expect to find the lesion on the second projection in an arc delineated with that distance as a radius ( Fig. 4 )
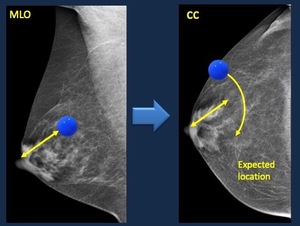
Fig. 4: Arch method. The distance from the nipple to the lesion on one projection, is the radius of the arch employed to find the lesion on the second projection.
• Additional views:
The use of additional views helps in work-up of image findings.
-Spot compression with or without magnification.
Spot compression views focalize on a suspicious image ( Fig. 5 ):
- A true lesion persists on spot compression views,
and the shape and margins are better depicted.
- Distortions are usually better depicted on spot compression views.
- Images caused by normal tissue usually disappear on spot compression.

Fig. 5: Mammogram. Focal asymmetry on right upper outer quadrant.
Spot compression view. It persists depicting irregular margin and spiculation. BIRADS 4 C.
Core biopsy Histopathology. Ductal infiltrating carcinoma
However several PITFALLS may appear on spot compression views,
which we should recognize in order to avoid them ( Fig. 6 ):
• Confirm that the image is included in the spot compression area.
It may be out from the area or too peripheral,
and then compression is not always effective .
• Thinning or disappearance on spot compression does not completely exclude malignancy.
Real lesions sometimes may appear less dense or “disappear” on spot compression,
due to low density or changes on superimposed breast tissue.

Fig. 6: Spot compression. Pitfalls.
Mammogram oblique view . Asymmetry on upper quadrant. Spot compression view is not correctly centered and the image is not clearly depicted. The lesion is evident on repeated correct spot compression with mass appearance. Core biopsy: infiltrating carcinoma.
- Different projections.
Mediolateral view:
In images depicted on mediolateral oblique view the use of an additional mediolateral view,
may help by confirming that the image is still evident,
and in determining its location on the orthogonal view (Fig. 7).
-Lesions located medially “move upwards” on the mediolateral view relative to the mediolateral oblique view.
-Lesions located laterally “move downwards” on the mediolateral view relative to the mediolateral oblique view.
-A lesion located centrally will not change location between the 90° lateral and MLO views

Fig. 7: Lateral views.
Mammogram Distortion on right inner upper quadrant. On lateral view the image moves upwards with respect to mediolateral oblique view
Rolled views:
In lesions visible only on craniocaudal view rolling the breast helps (Fig. 8):
-In determining if the image is real,
as different density appears by changing the position of superimposed fibroglandular tissue.
-Lesion location.
Lesions located in the upper quadrants move with the upper part of the breast to the medial and to the lateral side,
and so do lesions in the lower area.

Fig. 8: Rolled views. Mammogram CC view . Asymmetry visible on CC view, not depicted on oblique views.
The image disappears on rolled view, indicating it is caused by normal breast tissue.
4.2 Type of asymmetry.
Once it is confirmed that an image is real, the type of asymmetry should be determined.
• Visible on only one mammographic projection: Asymmetry.
• Visible on two mammographic projections:
- Large area (at least one quadrant).
Global asymmetry.
- Small area (less than one quadrant).
Focal asymmetry.
- Compare with previous. Focal asymmetry which is new,
larger or more conspicuous than on previous studies.
Developing asymmetry.
4.3. Asymmetry vs.
Mass.
An asymmetry or focal asymmetry may also be caused by a mass.
The use of additional exams (US,
MR,
tomosynthesis) may help in confirming whether the image corresponds to a mass ( Fig. 9 Fig. 10 Fig. 11 ).

Fig. 9: Asymmetry vs. Mass
-Asymmetry.
• Unilateral areas of fibroglandular tissue.
• Concave-outward borders.
• Interspersed with fat.
-Mass
• Space occupying 3-dimensional lesion.
• Convex-outward borders.
• Denser in the center than in the periphery (no fat within the lesion).

Fig. 10: Assymetry vs mass. Additional studies
50 yo woman. Asymptomatic.
Screening Mammogram . Dense breasts. Focal asymmetry (arrow).
Tomosynthesis. Multiple ill-circumscribed masses.
Radiological diagnosis: BIRADS 4C.
Core biopsy. Multicentric infiltrating ductal carcinoma

Fig. 11: Assymetry vs mass. Additional studies 50 yo woman.
Screening Mammogram: Focal asymmetry on upper outer quadrant of left breast
US demonstrates a mass. Core biopsy. Fibroadenoma
4.4. Differential diagnosis of asymmetric findings.
Work-up should continue trying to find out which entity is causing the image you have detected and analyzed.
4.4.1. First review clinical history: exclude surgery.
A history of previous surgery may be a cause for asymmetry,
focal asymmetry or global asymmetry.
The distribution of fibroglandular tissue becomes heterogeneous and a scar,
hematoma or fat necrosis may also appear (Fig. 12).

Fig. 12: Clinical history. Exclude surgery.
Mammogram. Asymmetry in a patient with a history of previous surgery.
US depicts a hypoechoic nodule consistent with fat necrosis.
4.4.2. Look for associated findings.
Presence of other imaging findings is important.
In cases of asymmetry,
focal,
global or developing asymmetry with microcalcifications or architectural distortion,
judge the lesion by its most suspicious findings (Fig. 13).

Fig. 13: Associated findings. Mammogram. Focal asymmetry with heterogeneous microcalcifications, better depicted on magnified view.
US . Hypoechoic area. BIRADS 5. MR confirmed a non-mass enhancing lesion. Core biopsy. Ductal infiltrating carcinoma.
4.4.3. Additional imaging.
Several additional imaging are usually required for evaluation of a single image or architectural distortion,
judge the lesion by its most suspicious findings (Fig. 14).

Fig. 14: Diagnostic work-up. Several additional studies are usually employed in diagnostic work-up for one individual lesion.
Screening mammogram: Focal asymmetry on lower inner quadrant of left breast.
Spot compression: It persists, so it is real, and we detect spiculated margins: Suspicious lesion.
US. 5-mm nodule. A needle was placed in the nodule under US control . Repeated mammogram with the needle in place confirms the nodule is causing the focal asymmetry, it appears on lateral view at the union of inner quadrants. Core biopsy: ductal epithelial hyperplasia and 1-mm focus of ductal infiltrating carcinoma.
US should be the first additional imaging.
Absence of US lesion does not exclude malignancy,
due to the fact that in lobular tumors cells may grow in sheets resembling normal breast tissue.
US may guide biopsy when a lesion is detected,
but in suspicious cases without US findings stereotactic biopsy should be performed.
Tomosynthesis is also useful in evaluation of asymmetries,
and may also help with tomosynthesis guided biopsy.
MR is not indicated as the initial evaluation in asymmetry work-up but it may have a role in suspicious images.
4.4.4. Causes for each type of asymmetry.
The causes which are more frequent for different types of asymmetry are:
• Asymmetry.
Asymmetry is most frequently due to summation artifact caused by overlapping tissue (Fig. 15). Changes in breast tissue composition owing to hormone replacement therapy,
weight loss,
or weight gain may also appear as an asymmetry.
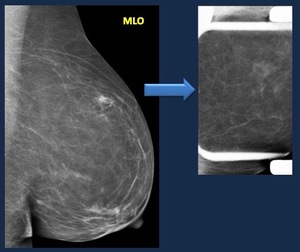
Fig. 15: Asymmetry. Causes. Mammogram. Asymmetry detected on oblique view, not visible on CC view.
On Spot compression view the image is dissociated.
Diagnosis. Normal breast tissue
It is only rarely malignant,
most often infiltrating lobular cancer due to the typical growth pattern of these subtype,
but also other malignancies such as lymphoma ( Fig. 16 ).

Fig. 16: Asymmetry. Causes. 76 yo w. Palpable lump on right breast.
Mammogram. Asymmetry on right upper quadrant visible only on oblique view.
On US heterogeneous, predominantly hyperechoic ill-circumscribed area on right upper outer quadrant. No axillary lymphadenopathy were found.
Core biopsy. MALT lymphoma.
Associated findings such as calcifications,
a palpable abnormality,
or architectural distortion should be detected as any such finding increases the suspicion of a malignancy.
Complete work-up is important,
sometimes a presumed Asymmetry turns into Focal asymmetry which is more frequently caused by ductal carcinoma ( Fig. 17 ).
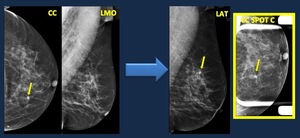
Fig. 17: Asymmetry. Causes. 58 yo woman. Follow-up in a patient with a history of ovarian cancer.
Mammogram. Asymmetry detected on CC view, not visible on Oblique view.
Image work-up: The image in evident on lateral view and persists on Spot compression view, so description should be changed to “focal asymmetry”.
US. No findings. Stereotactic biopsy was performed. Pathology. Ductal infiltrating carcinoma
• Global asymmetry.
It is most often a normal variant ( Fig. 18 ), and changes in breast tissue composition owing to hormone replacement therapy,
weight loss,
or weight gain may also cause global asymmetry.
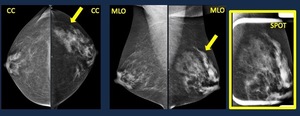
Fig. 18: Global Asymmetry. Causes. Mammogram. Global asymmetry on left breast.
No distortion nor microcalcifications on spot compression view. Normal asymmetric breast tissue
If palpable,
new,
distorted architecture or calcifications appear it may be malignant.
• Focal asymmetry
Most common causes are:
-Normal variant,
superimposition of normal breast ( Fig. 19 ).
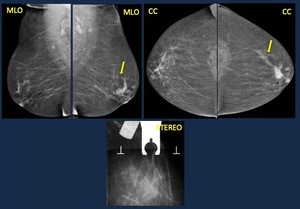
Fig. 19: Focal Asymmetry. Causes. 60 yo woman.Screening mammogram. Focal asymmetry.
On spot compression view it dissociates, although it partially persists.
Stereotactic core biopsy was performed.
Histopathology: normal breast tissue.
-A mass.
Spot compression and US may help in diagnosis ( Fig. 20 ).
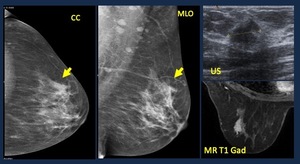
Fig. 20: Focal Asymmetry. Causes. 62-yo woman. Screening mammogram. Focal asymmetry. US. solid hypoechoic lobulated mass with slight acoustic shadowing. MR. Isointense mass with gadolinium enhancement.
Path. Ductal infiltrating carcinoma
Benign entities may present with focal asymmetry,
most frequently those with a diffuse growth such as inflammatory lesions : granulomatous mastitis (Fig. 21),
diabetic mastopathy or Pseudoangiomatous stromal hyperplasia (PASH).
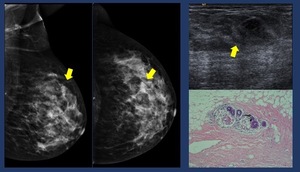
Fig. 21: Granulomatous mastitis. 29 yo woman. Palpable lump.
Mammogram. Focal asymmetry. US. Heterogeneous area with tubular hypoechoic structures. Core biopsy. Granulomatous mastitis.
Focal asymmetry may also be malignant,
more common if palpable,
new,
distorted architecture or calcifications appear.
Lobular carcinoma may present with focal asymmetry due to diffuse growth pattern,
but ductal carcinoma may also cause focal asymmetry.
In certain cases tomosynthesis or stereotactic core biopsy may help in diagnosis ( Fig. 22 ).

Fig. 22: Focal Asymmetry. Causes. Mammogram. Focal asymmetry on left upper outer quadrant.
On spot compression view it is barely visible. Tomosynthesis depicts spiculated 3 mm lesion.
Stereotactic core biopsy was performed. Histopathology: Ductal infiltrating carcinoma
• Developing asymmetry
It represents a focal asymmetry which is more evident than in precious studies,
so it is more often malignant,
either invasive lobular or ductal carcinoma,
DCIS or both ( Fig. 23 ).

Fig. 23: Developing Asymmetry. Causes. 69 yo woman. Screening mammogram. Developing asymmetry. An asymmetry not present on previous exam appears on oblique mammogram. US depicts an area of subtle acoustic shadowing. Radiological diagnosis: BIRADS 4C. Stereotactic vacuum-assisted biopsy was performed. Pathology: Grade 1 ductal infiltrating carcinoma.
But hormonal replacement treayment is also a frequent cause of developing asymmetry ( Fig. 24 ).

Fig. 24: Developing Asymmetry. Causes. 40 yo woman. Levonorgestrel- releasing intrauterine device hormonal treatment started in 2011. 2010 normal mammogram. 2013: Developing asymmetry on mammogram. Normal US. Discontinue treatment, and follow-up. 2014. Focal asymmetry persists less dense Diagnosis. Normal breast parenchyma, hormonal response.
Treatment should be discontinued and mammogram repeated in 3 months.
Any lesions able to appear as focal asymmetry may cause a developing asymmetry such as Pseudoangiomatous stromal hyperplasia ( Fig. 25 ).
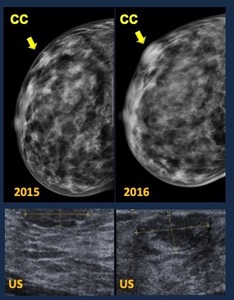
Fig. 25: Developing Asymmetry. Causes.
30 yo woman. Growing palpable lump
Mammogram 2015. Focal asymmetry Mammogram 2016. a mass is depicted
US. Heterogeneous ovoid mass, partially circumscribed margins
Radiological diagnosis. BIRADS 4B.
Core biopsy. Normal breast parenchyma. Microscopic foci of Pseudoangiomatous stromal hyperplasia.
Surgical specimen: Pseudoangiomatous stromal hyperplasia (PASH)
Developing asymmetries should be investigated to exclude malignancy,
unless a clearly benign cause is present.
4.4.5. Tips and tricks.
• Comparison with previous studies is important to detect developing asymmetries,
which are more frequently malignant.
• Remember normal variant in patients with hormonal therapy.
Treatment should be discontinued and mammogram repeated in 3 months.
• Thinning or disappearance on spot compression does not completely exclude malignancy.
• Absence of US lesion does not exclude malignancy.




 is not visible on CC view. A forced CC view depicts the lesion (arrow). MR confirms the enhancing nodule. Core biopsy. Infiltrating ductal carcinoma")






.
Tomosynthesis. Multiple ill-circumscribed masses.
Radiological diagnosis: BIRADS 4C.
Core biopsy. Multicentric infiltrating ductal carcinoma")














")