ECR 2019 / C-0753
Superior mesenteric artery: The vessel forgotten in the abdominal Doppler evaluation
Congress:
ECR 2019
Poster Number:
C-0753
Type:
Educational Exhibit
Keywords:
Abdomen, Arteries / Aorta, Vascular, Ultrasound-Colour Doppler, Ultrasound-Power Doppler, Ultrasound-Spectral Doppler, Education, Normal variants, Screening, Education and training, Obstruction / Occlusion, Image registration
Authors:
J. B. Rolleri Fajardo1, C. M. LIMA CONDO1, J. P. Mattocio Vevenis2; 1La Plata, Buenos Aires/AR, 2La Plata/AR
DOI:
10.26044/ecr2019/C-0753

Fig. 8:
FINDINGS AND DETAILS OF THE PROCEDURE
.")
Fig. 9:
Abdominal ultrasound B-mode, transverse section. Celiac artery trunk is easily...
.")
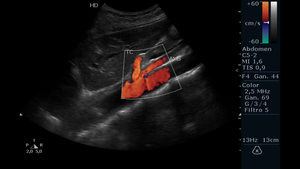
Fig. 10:
Abdominal ultrasound in power Doppler mode, transverse section. Celiac artery...
 and the distance between the anterior wall of the aorta to the posterior wall of the SMA two centimeters from the ostium. Abdominal aorta is observed.")
Fig. 11:
Abdominal ultrasound B-mode. Longitudinal section. Measurement of the exit...

Fig. 12:
Abdominal ultrasound in longitudinal section with spectral color Doppler...

Fig. 13:
Abdominal ultrasound in longitudinal section with spectral color Doppler...

Fig. 14:
COMMON FINDINGS

Fig. 15:
FINDINGS IN SMA
 of the SMA is observed.")
Fig. 16:
Abdominal ultrasound in mode B. Oblique longitudinal section. Parietal atheroma...
 with endoluminal echogenic image in the proximal third of it, which narrows the vessel lumen, compatible with SMA stenosis are visualized. AO indicates abdominal aorta.")
Fig. 17:
Abdominal ultrasound with evaluation in power Doppler mode. Longitudinal...

Fig. 18:
Abdominal ultrasound in B-mode, performing a longitudinal section where it is...

Fig. 19:
Abdominal ultrasound in color Doppler mode. Longitudinal section showing the...

Fig. 20:
Abdominal ultrasound in power Doppler mode, performing a longitudinal section...
 is recognized in the proximal third of the SMA. The PSV is increased, suggesting a significant stenosis.")
Fig. 21:
Abdominal ultrasound in longitudinal section with spectral color Doppler...

Fig. 22:
Abdominal ultrasound in longitudinal section with spectral color Doppler...
, SMA (AMS) and aortic.")
Fig. 23:
Abdominal ultrasound B-mode. Transverse section showing the LRV (Arrow), SMA...