ESHRE/ ESGE classifications system of female genital tract congenital anomalies
The newest classification system of female genital tract congenital anomalies is formed by the European Society of Human Reproduction and Embryology (ESHRE) and the European Society for Gynaecological Endoscopy (ESGE) under the name of a common working group called CONUTA (CONgenital UTerine Anomalies),
which published in 2013 the final version of the system.
This classification is mainly clinically oriented and anatomy based.
The main classes of the system summarize and group embryological maldevelopment according to the main types of fetal defects.
Variations in the anatomical presentation of the main classes form their subclasses.
In contrast to the oldest AFS system,
in this categorization cervical and vaginal anomalies are classified separately.
MRI (Magnetic resonance imaging) is the best noninvasive verifying imaging modality,
which demonstrates in detail anatomical deviations from the embryological origin of the female reproductive organs.
„Class U0 incorporates all cases with a normal uterus. A normal uterus is any uterus having an either straight or curved interostial line but with an internal indentation at the fundal midline not exceeding 50% of the uterine wall thickness.“ (Fig.1)
∗ Uterine wall thickness is the distance between the line connecting the tubal ostia (interostial line) and the external uterine profile at the midcoronal plane of the uterus.
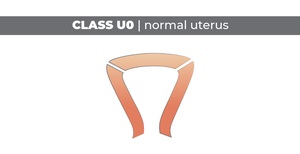
Fig. 1: Class U0 - normal uterus
On our first MRI example (Fig.2) we represent a normal uterus with the right position for measurement of the uterine wall thickness according to the definition above.
“Class U1 or Dysmorphic uterus incorporates all cases with a normal uterine outline but with an abnormal shape of the uterine cavity excluding septa." It is caused by late developmental embryological defects.
(Fig.3)
a) Subclass U1a or T-shaped uterus characterized by a narrow uterine cavity due to thickened lateral walls with a correlation 2/3 uterine corpus and 1/3 cervix.
b) Subclass U1b or uterus infantilis characterized also by a narrow uterine cavity without lateral wall thickening and an inverse correlation of 1/3 uterine body and 2/3 cervix.
c) Subclass U1c or others which is added to include all minor deformities of the uterine cavity including those with an inner indentation at the fundal midline level of <50% of the uterine wall thickness.
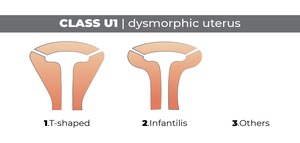
Fig. 3: Class U1 - dysmorphic uterus
On our second MRI example (Fig.4) we represent a case of uterus arcuatus according to the old AFS classification,
which can be included in the subclass U1c with an inner indentation at the fundal midline level <50% of the uterine wall thickness.
On our next example (Fig.5) we show a hypoplastic uterus with a long cervix on sagittal plane which could be an uterus infantilis.
“Class U2 or septate uterus incorporates all cases with normal fusion and abnormal (re)absorption of the midline septum.
Septate is defined as the uterus with a normal outline and an internal indentation at the fundal midline exceeding 50% of the uterine wall thickness.”(Fig.6)
a) Subclass U2a or partial septate uterus characterized by the existence of a septum dividing partly the uterine cavity above the level of the internal cervical os
b) Subclass U2b or complete septate uterus characterized by the existence of a septum fully dividing the uterine cavity up to the level of the internal cervical os.
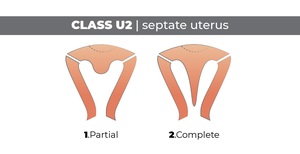
Fig. 6: Class U2 - septate uterus
In Fig.7 and Fig.8 we show two cases of complete septate uterus class U2 subclass b – first one as an incidental finding in a 96 years old woman and a second one of a 58 years old woman.
“Class U3 or bicorporeal uterus incorporates all cases of fusion defects.
As bicorporeal is defined the uterus with an abnormal fundal outline; it is characterized by the presence of an external indentation at the fundal midline exceeding 50% of the uterine wall thickness.”(Fig.9)
а) Subclass U3a or partial bicorporeal uterus characterized by an external fundal indentation partly dividing the uterine corpus above the level of the cervix.
b) Subclass U3b or complete bicorporeal uterus characterized by an external fundal indentation completely dividing the uterine corpus up to the level of the cervix.
C) Subclass U3c or bicorporeal septate uterus - combined defect characterized by a width of the midline fundal indentation exceeding 150% the uterine wall thickness.
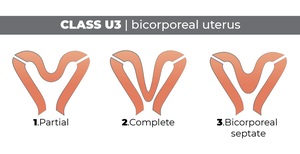
Fig. 9: Class U3 - bicorporeal uterus
On the next two cases,
we represent both women with bicorporeal uterus – the first one (Fig.10) with double "normal" cervices (C2 anomaly) and the second one (Fig.11) with unilateral aplasia of the cervix (C3 anomaly).
“Class U4 or hemi-uterus incorporates all cases of a unilaterally formed uterus; the contralateral part could be either incompletely formed or absent.
It is a formation defect.”(Fig.12)
a) Subclass U4a or hemi-uterus with a rudimentary (functional) cavity – unicorn uterus with communicating or non-communicating functional contralateral horn.
b) Subclass U4b or hemi-uterus without rudimentary (functional) cavity – unicorn uterus without non-functional contralateral uterine horn or by aplasia of the contralateral part.
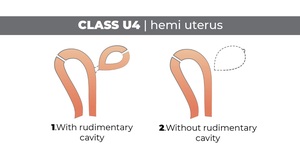
Fig. 12: Class U4 - hemi-uterus
On the next two images below we show our cases of hemi-uterus with (Fig.13) and without (Fig.14) a rudimentary cavity.
In the first one,
we have a case of genetically proved Herlin-Werner-Wunderlich syndrome (OHVIRA = obstructive hemivagina with ipsilateral renal anomaly).
This patient has also right renal agenesis.
“Class U5 or aplastic uterus incorporates all cases of uterine aplasia.
It is a formation defect” (Fig.15)
a) Subclass U5a or aplastic uterus with rudimentary (functional) cavity - characterized by the presence of bi- or unilateral functional horn.
b) Subclass U5b or aplastic uterus without rudimentary (functional) cavity - characterized either by the presence of uterine remnants or by full uterine aplasia.”
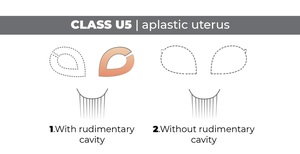
Fig. 15: Class U5 - aplastic uterus
In the next two videos (Fig.16 and Fig.17),
we show a case of Mayer-Rokitanski-Kusler-Hauser syndrome - type 1.
Our patient has complete congenital uterine aplasia (class U5 subclass b) with partial vaginal aplasia (subclass V4 anomaly) with a lack of association with other non-Mullerian anomalies.
This young woman complained of primary amenorrhoea.
“Class U6 or unclassified cases…infrequent anomalies,
subtle changes or combined pathologies could not be allocated correctly to one of the six groups; Duplication defects or ectopic Müllerian tissue anomalies […] could be put in this class".
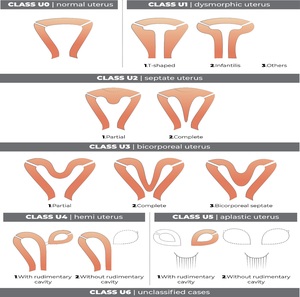
Fig. 18: Summary of the uterine anomalies according to ESHRE/ESGE classification of female genital tract congenital anomalies - nomenclature, classes & subclasses;
Clinical presentation & reproductive consequences
Congenital anomalies of the female genital tract have a common prevalence of 3-6% of the female population and can cause gynecological problems and reproductive disorders in young women.
They can be asymptomatic until puberty and appear for the first time like primary amenorrhea or with cyclic pelvic pain.
Infertility and increased risk of obstetric complications are other serious clinical consequences.
There is an association with other "non-Mullerian" congenital anomalies,
because of the common urinary and genital embryological origin.
Therapy
For uterine anomalies could be used surgical methods like hysteroscopic septal resection or abdominal metroplasty a modo Strassman,
but all of them are appropriate only in symptomatic women with no other cause of infertility found.








 syndrome")

