ECR 2019 / C-1015
A practical guide for a correct staging of renal cancer: what urologists want to know
Congress:
ECR 2019
Poster Number:
C-1015
Type:
Educational Exhibit
Keywords:
Neoplasia, Multidisciplinary cancer care, Surgery, Structured reporting, CT, Kidney, Genital / Reproductive system male
Authors:
F. Rosa1, I. Verardo1, S. Barbagallo1, G. Perugin1, C. Martinetti2, L. Basso1, L. Secondini1, S. Sanguinetti1, C. E. Neumaier1; 1Genova/IT, 2Genoa/IT
DOI:
10.26044/ecr2019/C-1015

Fig. 4:
PADUA score

Fig. 5:
R.E.N.A.L. scoring system

Fig. 6:
C-INDEX scoring system

Fig. 7:
POLAR LINE VS SINUS LINE DEFINITION.
In coronal plan: Polar line is designated...

Fig. 8:
clinical cases

Fig. 9:
clinical cases

Fig. 10:
clinical cases

Fig. 11:
Clinical cases, same patient of figure 10: CT showed also two anatomic variant.

Fig. 12:
Arterial anatomic variants

Fig. 13:
Venous anatomic variants
 MDCTI allowed identification of collateral feeding vessel from the surrenalic artery (Yellow arrows, C) and artero-venous shunt with venous ectasia (red arrow in B).")
Fig. 14:
Advanced right renal lesion (*) MDCTI allowed identification of collateral...

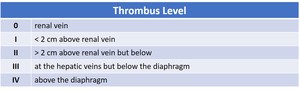
Fig. 15:
Tumor Thrombus level

Fig. 16:
Tumor Thrombus: level I

Fig. 17:
Tumor Thrombus: level I.

Fig. 18:
Tumor Thrombus: level II.

Fig. 19:
Tumor Thrombus: level II

Fig. 20:
Tumor Thrombus: level III.

Fig. 21:
Tumor Thrombus: level IV.

Fig. 22:
Tumor Thrombus: level IV.

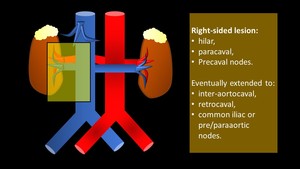
Fig. 23:
Right-sided tumors nodal dissection: hilar, paracaval, and precaval nodes, with...

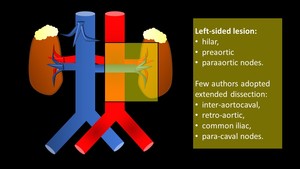
Fig. 24:
Left-sided tumor nodal dissetion: hilar, preaortic and paraaortic nodes, with...

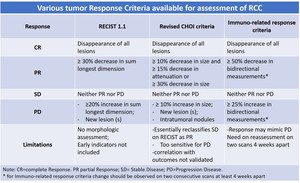
Fig. 25:
Some tumor Response Criteria available for assessment of RCC

Fig. 2:
TNM 8th edition