Review of elbow anatomy and function
Anatomy
The elbow is a synovial joint composed of three articulations.
The humeroradial articulation is formed between the capitellum of the humerus and the radial head,
while the humero-ulnar articulation is formed between the trochlea of the humerus and the trochlear notch of the ulna. The radial head and the radial notch of the ulna form the radioulnar articulation.
It is enclosed by the fibrous layer of the joint capsule while the synovial membrane lines the internal surface of the fibrous layer.
Thickenings of the fibrous layer of the joint capsule form the medial and lateral collateral ligaments which provide stability.
The lateral collateral ligament covers and stabilizes the head of the radius in the radial notch of the ulna. The medial collateral ligament runs from the medial epicondyle of the humerus to the coronoid process and olecranon of the ulna.
The anterior and posterior fat pads are located deep to the capsular margins. The elbow also contains the superficial olecranon bursa located over the olecranon process and the bicipitoradial bursa located between the distal biceps tendon the radial tuberosity.
[4] Fig. 1

Fig. 1: Anatomy review. Elbow radiograph, PA and lateral views.
Function
The elbow joint is a hinge and pivot joint which allows for flexion and extension to occur. The humero-ulnar articulation composes the hinge and allows for up to 170 degrees of extension.
[9] The humeroradial and proximal radioulnar joints forms the pivot component which allows pronation and supination at the elbow joint.
Imaging techniques
Conventional radiography is preferred for initial routine imaging of the elbow.
To evaluate a patient for bone abnormalities and associated fractures it is necessary to obtain anteroposterior,
lateral and oblique views of the elbow. Proper positioning for the AP view includes a fully extended elbow with supination of the forearm,
assuring visualization of the medial and lateral epicondyles,
radiocapitellar joint,
and measurement of the carrying angle.
[4] Proper positioning of the lateral view includes the elbow flexed to 90 degrees with the forearm in neutral position,
allowing visualization of the ulnotrochlear joint,
coronoid process and the olecranon process.
Multidetector Computed Tomography (MDCT) is used following conventional radiographies of the elbow to further evaluate complex fractures.
[5]
Elbow fractures and mechanisms of injury
Adults
Proximal radius: 33-50% of all elbow fractures seen in adults,
most common elbow fracture.
Mechanism of injury is usually caused by axial loading when falling on an outstretched hand with elbow extension and forearm pronation.
This causes the radial head to collide with the capitelllum of the humerus.
The most used classification is the Mason-Johnston system which has four divisions.
Type I refers to non-displaced fractures or fractures with < 2 mm of displacement.
Type II injuries are those displaced < 2 mm or that present with angulated fracture fragment.
Type III injuries are comminuted proximal radial fractures.
Lastly,
type IV injuries require a combination of radial head fracture with dislocation.
Radiological report should include description of displacement,
articular surface injured,
if there is comminution and if dislocation occurred.
[12] Fig. 2, Fig. 3

Fig. 2: Left elbow lateral (A) and AP (B) views with depressed fracture of the anterior surface of the radial head (teal arrows). Mason-Johnston type I injury. Associated hemarthrosis and soft tissue swelling. No dislocation.
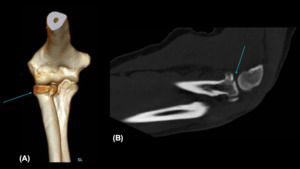
Fig. 3: Right elbow volume-rendered CT 3D reconstruction (A) and sagittal bone window CT (B) showing a comminuted, intra-articular depressed fracture of the anterolateral aspect of the radial head (teal arrows), with slight bone impaction, fracture lines extend into the radial-capitellar and radioulnar joints surfaces. There is no elbow joint dislocation. Mason-Johnson type III injury.
Distal humerus: Most common mechanisms are falling on an outstretched hand and axial loading to the humerus on a flexed elbow.
The most used system to classify these fractures is from the Swiss Arbeitsgemeinschaft für Osteosynthesefragen-Association for the Study of Internal Fixation (AO-ASIF).
It is divided in three types: Type A injures are extra-articular fractures,
type B are partial articular fractures,
and type C are complete articular fractures with involvement of both columns. Radiological report should include information about column involvement,
articular extension,
description of displacement and if there is comminution.
[12] Fig. 4, Fig. 5
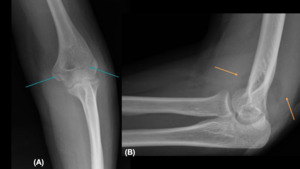
Fig. 4: AP (A) and lateral (B) radiographs of the left elbow showing a fracture through the bilateral humeral epicondyles/distal humerus (teal arrows). There are anterior and posterior fat pad signs (orange arrows), as may be seen with joint effusion/hemarthrosis.
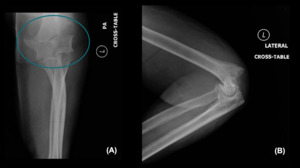
Fig. 5: Left elbow radiograph, PA (A) and lateral (B) views showing a comminuted transcondylar fracture of the distal humerus, with intra-articular extension and anterior displacement and overriding of the major distal fragment (teal circle). The radial head suggests to be dislocated with respect to the capitellum. Soft tissue swelling is associated to fracture.
Coronoid process: mostly seen in cases of elbow dislocation.
Axial loading to a flexed elbow,
usually when falling on an outstretched hand,
is a common mechanism.
The O’ Driscoll classification is frequently used and is divided in three types: type I which is coronoid tip fractures,
type II which have anteromedial facet disruption and type III which are fractures of the base of the coronoid process that involve more than 50% of the coronoid body.
Radiological report should include the size of the fractured fragment,
if there is involvement of the anteromedial facet and of the coronoid base.
[12] Fig. 6 , Fig. 7

Fig. 6: Left elbow radiographs AP (A) and lateral (B) views showing posterior dislocation of the radius and ulna. Additionally, radial head and coronoid process fractures are suggested.
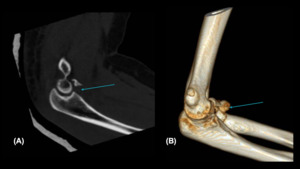
Fig. 7: Left elbow CT sagittal bone window (A) and sagittal volume-rendered 3D reconstruction with a communited fracture of the coronoid process. Additional fractures included: intra-articular compression fracture of the radial head with more than to thirds involvement of the articular surface and the a slightly depressed fracture fragment; avulsion fracture of the medial epicondyle likely from both common extensor tendon avulsion and ulnar collateral ligament avulsion injury; and avulsion fracture of the humeral attachment of the radial collateral ligament.
Olecranon: can be seen in different injury mechanisms such as vertical stress to humerus when elbow has a 90-degree flexion,
hyperextension injuries,
or contraction of the brachialis and triceps in opposite directions.
Radiological report should include measurement of the displacement and if there is comminution.
[12] Fig. 8, Fig. 9, Fig. 10
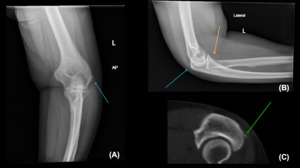
Fig. 8: AP (A) and lateral (B) views with cortical disruption at the anterior aspect of the radial head/neck suggesting a nondisplaced fracture. A thin linear density is projecting in the soft tissues adjacent to the olecranon process. Reconstructed CT image (C) demonstrates an osseous fragment posterior to the olecranon process of the ulna.
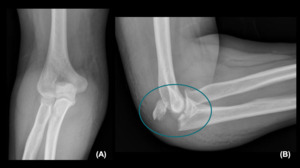
Fig. 9: PA (A) and lateral (B) views of the right elbow showing a displaced/distracted fracture of the olecranon with intra-articular extension that appears to be comminuted (teal circle).
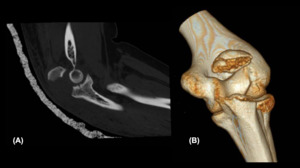
Fig. 10: Right elbow CT sagittal bone window (A) and coronal volume-rendered 3D reconstruction showing a comminuted distracted fracture of the olecranon with intra-articular extension. Distracted fragment is displaced approximately 1.7 cm superiorly with superior angulation. No dislocations.
Elbow dislocations: second most commonly dislocated joint in adults.
They are usually caused when falling on an outstretched hand with either axial loading on a hyperextended elbow or axial loading with supination and valgus stress.
Simple elbow dislocations are those with isolated capsuloligamentous injury.
The complex dislocations require a fracture component.
A dislocation classified as divergent must have the humerus lying between the radius and ulna after trauma.
[12,
15] Fig. 11, Fig. 12
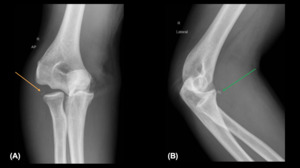
Fig. 11: PA (A) and lateral (B) radiographs of the right elbow showing dislocation of the radius and ulna with respect to the humerus. Calcific densities are projecting adjacent to the radial head (orange arrow) which are believed to represent bone fragments of unclear donor site. Fracture of the coronoid process of the ulna is suspected (green arrow).
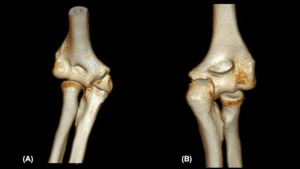
Fig. 12: AP (A) and PA (B) coronal CT volume-rendered 3D reconstructions showing medial dislocation of the olecranon and radial head. Additionally, there are fractures of the radial head, olecranon and coronoid process with intra-articular fracture fragments.
Terrible triad: Complex,
posterior elbow dislocation with associated radial head fracture and coronoid fracture is known as the terrible triad.
These injuries are associated to subsequent elbow joint instability,
subluxation and dislocations.
Also,
they are at increased risk of developing a compartment syndrome.
[3,
12] Fig. 13, Fig. 14, Fig. 15

Fig. 13: PA (A) and lateral (B) radiographs of the left elbow demonstrating posterior elbow dislocation, with associated comminuted/displaced fractures of the radial head/neck and coronoid process of the ulna. There is elbow hemarthrosis, as well as diffuse soft tissue swelling of the elbow and proximal forearm.
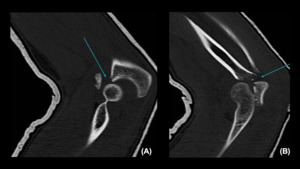
Fig. 14: Left elbow CT sagittal bone window reconstructions (A-B) with chip fracture of the ulna (teal arrow in A) and distracted/comminuted fracture of the radial neck/head (teal arrow in B) with posterolateral displacement of the main bone fragment. Additionally, there is complete dislocation of the elbow joint.
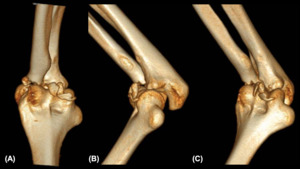
Fig. 15: Left elbow CT volume-rendered 3D images (A-C) showing complete dislocation of the elbow joint. Additionally, patient had a chip fracture of the coronoid process of the ulna and a distracted/comminuted fracture of the radial neck/head.
Monteggia: combination of ulnar fracture with radiocapitellar dislocation.
Most common mechanisms are direct impact to the ulnar bone or falling on an outstretched hand with forearm in pronation or hyperextension.
Classified by the Bado system.
In type I injuries there is ulnar fracture with anterior dislocation of the radial head.
An ulnar fracture combined with a posterior or posterolateral dislocation is considered a type II injury.
Type III has an ulnar fracture with a lateral or anterolateral radial head dislocation.
Lastly,
the type IV injury has ulnar and radial fractures with anterior dislocation of the radial head.
Radiological report should include description of the radial dislocation,
describe the angulation of the ulnar fracture fragment and mention if there are any radial fractures present.
[11,12] Fig. 16, Fig. 17
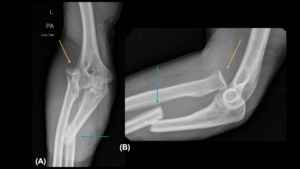
Fig. 16: PA (A) and lateral (B) radiographs of the left elbow showing an anterolateral dislocation of the radius with respect to the capitellum (orange arrows). There is a displaced angulated overriding fracture of the proximal ulna with associated bone fragments (teal arrows).
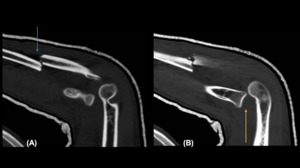
Fig. 17: Left elbow CT sagittal bone window reconstructions (A-B) showing a proximal third ulnar shaft fracture (teal arrow in A) and radial head cephalad dislocation (orange arrow in B).
Children
Supracondylar: most common elbow fractures in children.
Most common mechanisms are direct impact to the elbow in flexion or axial loading by falling on an outstretched hand when elbow is in hyperextension.
In the latter,
the olecranon process impacts the olecranon fossa of the humerus resulting in a supracondylar fracture.
The Gartland system is commonly used to classify these fractures.
Type I injures are those that are non-displaced or minimally displaced.
Type II are displaced fractures with a preserved cortex.
Finally,
type III fractures are displaced with associated cortical disruption.
[8] Fig. 18
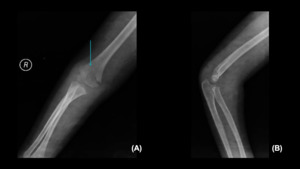
Fig. 18: Right elbow PA (A) and oblique (B) radiographs showing a minimally displaced supracondylar fracture (teal arrow) without significant displacement. No dislocations. There is faint visualization of anterior and posterior fat pads in keeping with hemarthrosis.
Lateral epicondylar: second most common elbow fracture in children.
The mechanism is usually due to a varus force caused by falling on an outstretched hand with forearm in supination.
The Milch classification is also used,
with type I fractures being those in the lateral metaphysis that extend into capitellar ossification center and type II extending into the capitellar-trochlear groove with an additional trochlear fracture.
[8] Fig. 19

Fig. 19: Left elbow PA (A) and oblique (B) radiographs showing a lateral humeral epicondylar fracture (teal arrows) with displacement.
Medial epicondylar: 10% of elbow fractures,
third most common in children.
They are usually associated to elbow dislocation.
Mechanism is a valgus force caused by falling on an outstretched hand.
[8]
Proximal radius: When there is a valgus stress caused by falling on an outstretched hand with forearm in hyperextension,
a proximal radial fracture may occur.
These are considered Salter-Harris type II which are fractures that cross the growth plate and reach the metaphysis.
[8] Fig. 20
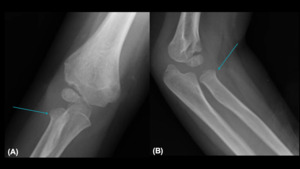
Fig. 20: AP (A) and lateral (B) radiographs of the right elbow showing a minimally impacted radial head fracture (teal arrows).
Elbow dislocation: To identify an elbow dislocation in pediatric population,
evaluate for radiocapitellar line disruption.
If necessary,
ultrasound of the elbow may be used.
These injuries usually result from a hyperextended forearm with varus stress.
They can be classified as an isolated radial head dislocation or as radioulnar dislocations with ulnar fracture,
also known as Monteggia fractures.
These can be further classified using the Bado system.
Anterior dislocations of the radial head with ulnar fractures are type I injuries.
An ulnar fracture combined with a posterior or posterolateral dislocation is considered a type II injury.
The type III has an ulnar fracture with a lateral or anterolateral radial head dislocation.
Lastly,
the type IV injury has ulnar and radial fractures with anterior dislocation of the radial head.
[8,
11] Fig. 21
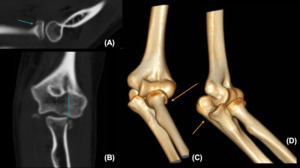
Fig. 21: Left elbow CT sagittal bone window (A), coronal bone window (B) and 3D volume-rendered reconstructions (C-D) showing a comminuted fracture of the anterolateral aspect of the radial head (teal arrows). There is medial dislocation of the radiocapitellar joint and coronoid process with rotatory/supination component of the coronoid process in relationship with the trochlea (orange arrows).
Management
Radial head and neck
Management is targeted for joint and mobility preservation and it is mostly based on the degree of angulation.
Nonoperative management,
is usually the first line in treatment.
Injuries in children involving less than 30 degrees angulation are candidates for long arm cast immobilization and short term follow up with early mobilization,
while injuries affected by more than 30 degrees angulation are routinely managed with surgical therapy.
[13]
Surgical management is mostly based on the degree of elbow instability and therapy is targeted to preserve stability.
In comminuted fractures,
there is a higher risk of concomitant ligamentous injury that should be known prior to intervention.
Closed percutaneous reduction and pinning is gaining praise since it provides the most benefit to younger patients due to the decreased risk of avascular necrosis,
synostosis,
heterotopic ossification,
infection,
and decreased range of motion.
[13,
14]
Distal humeral
Nonoperative management with cast immobilization is best suited for nondisplaced or minimally displaced epicondylar fractures.
Displaced epicondylar avulsions and two-column fractures are treated with open reduction and internal fixation in most cases,
as well as comminuted or two-column fractures.
[12] Nevertheless,
total joint arthroplasty may also be performed in elderly patients with comminuted fractures and arthritic changes.
Coronoid process
Due to the importance of the coronoid process for elbow stability after dislocations,
its presence or absence aids in guiding orthopaedic management. Coronoid process repair usually takes into consideration fragment size and fracture location for surgical planning.
[10] Nonoperative management of coronoid process fractures is indicated for injuries that are nondisplaced with a stable non-dislocated elbow.
Open reduction and internal fixation management is performed on all types of coronoid process fracture with associated elbow instability and when part of the “terrible triad”.
[16]
Olecranon
Immobilization for olecranon fractures is best suited for patients with nondisplaced fractures or displaced fractures in people who do not require full mobility.
Operative management aims to individualize patient care with surgical techniques being dependent on the type of injury.
[6,
12]
Terrible triad
Rarely treated conservatively. The approach of surgical repair depends on the degree and combination of fractures and may include one or a combination of radial head replacement,
MCL and LCL repair,
and fixation of the coronoid fracture fragment.
The pattern and mechanism of injury will determine the manner of approach to the surgical intervention and elbow instability will be the final step analysed to determine whether an external fixator will be used.
[10]
Monteggia
Children are conservatively treated,
while adults require early surgical intervention in order to preserve stability and full range of motion.
Open reduction and internal fixation of the ulnar fracture may be performed in patients with unstable,
open,
or comminuted fractures while intramedullary rods are suited for transverse or oblique ulnar fractures.
[7]
Elbow dislocation
Stable,
simple dislocations nonoperative treatment in both adults and children.
Complex and divergent dislocations are indications for open reduction and internal fixation and may also be accompanied by LCL and MCL repair in unstable dislocations.
[2,
12]
Complications
Complications include: non-union or malunion of the fracture fragments,
decreased mobility,
and damage to adjacent structures,
especially the ulnar nerve.
[1]


 and AP (B) views with depressed fracture of the anterior surface of the radial head (teal arrows). Mason-Johnston type I injury. Associated hemarthrosis and soft tissue swelling. No dislocation.")
 and sagittal bone window CT (B) showing a comminuted, intra-articular depressed fracture of the anterolateral aspect of the radial head (teal arrows), with slight bone impaction, fracture lines extend into the radial-capitellar and radioulnar joints surfaces. There is no elbow joint dislocation. Mason-Johnson type III injury.")
 and lateral (B) radiographs of the left elbow showing a fracture through the bilateral humeral epicondyles/distal humerus (teal arrows). There are anterior and posterior fat pad signs (orange arrows), as may be seen with joint effusion/hemarthrosis.")
 and lateral (B) views showing a comminuted transcondylar fracture of the distal humerus, with intra-articular extension and anterior displacement and overriding of the major distal fragment (teal circle). The radial head suggests to be dislocated with respect to the capitellum. Soft tissue swelling is associated to fracture.")
 and lateral (B) views showing posterior dislocation of the radius and ulna. Additionally, radial head and coronoid process fractures are suggested.")
 and sagittal volume-rendered 3D reconstruction with a communited fracture of the coronoid process. Additional fractures included: intra-articular compression fracture of the radial head with more than to thirds involvement of the articular surface and the a slightly depressed fracture fragment; avulsion fracture of the medial epicondyle likely from both common extensor tendon avulsion and ulnar collateral ligament avulsion injury; and avulsion fracture of the humeral attachment of the radial collateral ligament.")
 and lateral (B) views with cortical disruption at the anterior aspect of the radial head/neck suggesting a nondisplaced fracture. A thin linear density is projecting in the soft tissues adjacent to the olecranon process. Reconstructed CT image (C) demonstrates an osseous fragment posterior to the olecranon process of the ulna.")
 and lateral (B) views of the right elbow showing a displaced/distracted fracture of the olecranon with intra-articular extension that appears to be comminuted (teal circle).")
 and coronal volume-rendered 3D reconstruction showing a comminuted distracted fracture of the olecranon with intra-articular extension. Distracted fragment is displaced approximately 1.7 cm superiorly with superior angulation. No dislocations.")
 and lateral (B) radiographs of the right elbow showing dislocation of the radius and ulna with respect to the humerus. Calcific densities are projecting adjacent to the radial head (orange arrow) which are believed to represent bone fragments of unclear donor site. Fracture of the coronoid process of the ulna is suspected (green arrow).")
 and PA (B) coronal CT volume-rendered 3D reconstructions showing medial dislocation of the olecranon and radial head. Additionally, there are fractures of the radial head, olecranon and coronoid process with intra-articular fracture fragments.")
 and lateral (B) radiographs of the left elbow demonstrating posterior elbow dislocation, with associated comminuted/displaced fractures of the radial head/neck and coronoid process of the ulna. There is elbow hemarthrosis, as well as diffuse soft tissue swelling of the elbow and proximal forearm.")
 with chip fracture of the ulna (teal arrow in A) and distracted/comminuted fracture of the radial neck/head (teal arrow in B) with posterolateral displacement of the main bone fragment. Additionally, there is complete dislocation of the elbow joint.")
 showing complete dislocation of the elbow joint. Additionally, patient had a chip fracture of the coronoid process of the ulna and a distracted/comminuted fracture of the radial neck/head.")
 and lateral (B) radiographs of the left elbow showing an anterolateral dislocation of the radius with respect to the capitellum (orange arrows). There is a displaced angulated overriding fracture of the proximal ulna with associated bone fragments (teal arrows).")
 showing a proximal third ulnar shaft fracture (teal arrow in A) and radial head cephalad dislocation (orange arrow in B).")
 and oblique (B) radiographs showing a minimally displaced supracondylar fracture (teal arrow) without significant displacement. No dislocations. There is faint visualization of anterior and posterior fat pads in keeping with hemarthrosis.")
 and oblique (B) radiographs showing a lateral humeral epicondylar fracture (teal arrows) with displacement.")
 and lateral (B) radiographs of the right elbow showing a minimally impacted radial head fracture (teal arrows).")
, coronal bone window (B) and 3D volume-rendered reconstructions (C-D) showing a comminuted fracture of the anterolateral aspect of the radial head (teal arrows). There is medial dislocation of the radiocapitellar joint and coronoid process with rotatory/supination component of the coronoid process in relationship with the trochlea (orange arrows).")