ECR 2019 / C-1105
Mechanical thrombectomy for ischemic anterior circulation stroke patients older than 80 years. A single center experience.
Congress:
ECR 2019
Poster Number:
C-1105
Type:
Scientific Exhibit
Keywords:
Acute, Thrombolysis, Recanalisation, Catheter arteriography, Vascular, Neuroradiology brain, Interventional vascular, Embolism / Thrombosis
Authors:
I. Oronoz Mitxelena1, O. Chirife1, R. Barranco Pons1, L. Aja Rodríguez1, M. A. De Miquel1, S. Aixut Lorenzo1, B. Lara1, H. Quesada García2, P. Cardona1; 1Barcelona/ES, 2L´Hospitalet de Llobregat (Barcelona) /ES
DOI:
10.26044/ecr2019/C-1105

Fig. 1:
Distribution plot of age.
.")
Fig. 2:
Distribution plot of ASPECTS and of baseline functional status (NIHSS).
.")
Fig. 3:
Distribution plot of recanalization (mTICI).

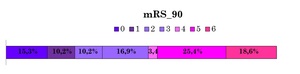
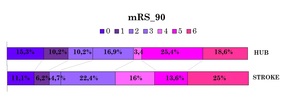
Fig. 4:
Scores on the modified Rankin Scale at 90 days. Distribution of scores at 90...

Fig. 5:
Distribution plot of hemorrhagic transformation.

Table 1:
Statistical analysis results, comparing the group that obtained mRS90 2 or...

Table 2:
Statistical analysis results, comparing the group that obtained mRS90 2 or...

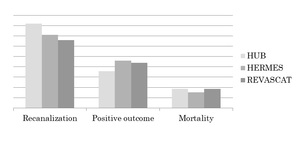
Fig. 6:
Successful recanalization rate, positive functional result and mortality rate...

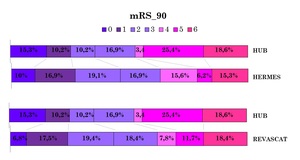
Fig. 7:
Scores on the modified Rankin Scale at 90 days. Distribution of scores at 90...

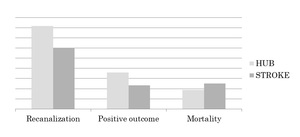
Fig. 8:
Successful recanalization rate, positive functional result and mortality rate...
.")
Fig. 9:
Scores on the modified Rankin Scale at 90 days. Distribution of scores at 90...