1- Definition of the non-atheromatous disease of the carotid vessels (NADCA): It is all carotid pathology that is not of atheromatous cause.
Atheromatous plaques and their complications,
such as stenoses or occlusions,
are excluded. It is important to know,
if the lesion is primary of the carotid space,
if it is vascular and if it is adjacent or intrinsic to the Internal Carotid Artery (ICA)6.
2- Etiologies: The NADCA etiologies involve a series of not so frequent entities such as congenital anomalies such as agenesis or hypoplasia and ectasia or dolichoarteriopathy disease. It also includes the arterial wall inflammatory or dysplastic pathologies such as Takayasu's or postradiation arteritis,
Carotidynia,
and fibromuscular dysplasia.
Moreover,
aneurysm,
pseudoaneurysms,
arteriovenous fistulas,
dissections and embolisms can be added.
We must not forget the tumor pathologies,
primary as the carotid Glomus,
or secondary.
3- Classification: There are no currently published classifications.
We propose grouping them according to those that affect the wall,
those that generate mass effect and others.
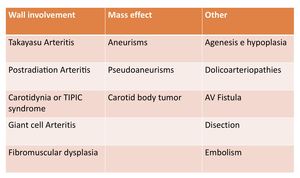
Fig. 1: Proposed classification of the non atheromatous pathology in the Carotid arteries. It can be group according the involvement of the arterial wall, the production of mass effect and others.
4. Sonographic appearance and signs:
4.A.
Congenital pathology: The congenital absence of the ICA is a very rare anomaly,
with an incidence lower than <0.01%3.
It can be bilateral,
but unilateral involvement is more frequent and more on the left side (3/1).
It is thought to be due to mechanical or hemodynamic disorder during embryonic development.
It is usually asymptomatic due to the compensatory collateral circulation and is detected incidentally in a radiological study.
The three main radiological findings are:
- decreased caliber or absence of visualization of the ICA,
partial or complete - absence or hypoplasia of the carotid canal in the temporal bone
- collateral circulation through the Willis polygon,
persistent embryonic arteries or transcranial vessels from the ACE.
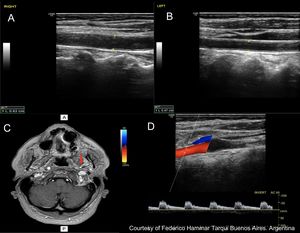
Fig. 2: Left ICA agenesis. A and B: A difference in size between the two common carotids is observed, with the left being smaller.
C: Brain Magnetic Resonance where the absence of internal carotid is observed.
D: Doppler spectrum of the external carotid artery, where flows of low resistance are observed, attributable to the derivation of flows in a collateral form towards the polygon of Willis.
Courtesy of Federico Hammar Tarqui. Buenos Aires. Argentina.
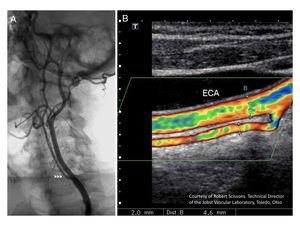
Fig. 3: Hypoplasia of the Internal Carotid Artery. A: Digital Angiography. B: Color Doppler Ultrtasound.
The ICA is significantly smaller than de External Carotid Artery.
4.B.
Ectasic carotid disease or dolichoarteriopathy: It is the elongation or change of angulation of the vessel,
forming unusual curves,
from congenital origin or acquired forms in diseases such as fibromuscular dysplasia (FMD),
arteriosclerosis or hypertension.
There is no difference between sexes or age,
they can be present even in children.
Their etiology is not clear.
They are usually asymptomatic,
or they present as murmurs or pulsatile masses at the neck.
However,
they can also be accompanied with TIA or stroke,
especially in elderly patients.
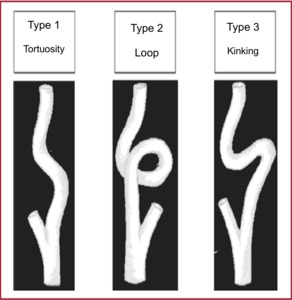
Fig. 4: Types of dolicoarteriopathies according to Weibel and Fields 1.
There are three types 1
- Type 1: Tortuosity: defined as a non-rectilinear path of an artery with kinks with angles greater than 90º.
- Type 2: Loop: is the angulation of an artery in 360º on its transversal axis,
resulting in a circular configuration.
- Type 3: Kink: is the inflection of one or more segments with an internal angle less than or equal to 90º.
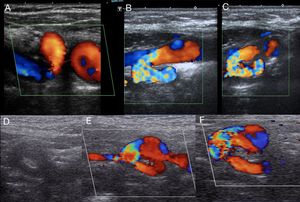
Fig. 5: Kinks and coils. Curvatures in the Carotis arteries
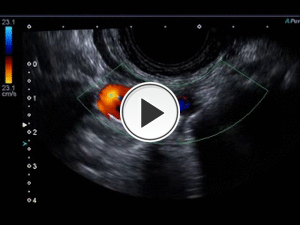
Fig. 6: Double bending of the distal internal carotid, visualized with a sectorial transducer that allowed reaching that challenging portion of the artery.
This type of double kinks can emulate the sign of the ¨S¨ described in association to fibromuscular dysplasia

Fig. 7: Pronounced kinking of the internal carotid, clinically evident as a pulsatile mass
Technically the bends complicate the angle positioning and the calculation of the velocities.
Already,
in the kinks,
high speeds are observed.
This complexity increases if there are also atheromatous plaques in the kinks.

Fig. 8: Important bend in the form of a fold of the internal carotid artery, which produces a marked increase in speeds at that level. It seemed to generate significant hemodynamic changes with parameters of stenosis greater than 70%
4.C.
Arteritis:
- Takayasu´s arteritis: It is a granulomatous vasculitis of unknown etiology that affects the aorta and supra-aortic trunks (Common Carotid and Subclavia).
It is characterized by the concentric thickening of the intima-media complex.
It can also affect the abdominal Aorta and its branches.
It also courses with segments of segmenal stenosis,
occlusion,
dilatation and/or aneurysm formation4.
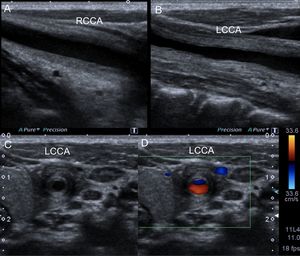
Fig. 9: Takayasu´s arteritis in a 11 years old boy. It started with severe episodic pain in the left part of the neck, with positive acute fase reactants. An increase in wall thickness, concentric and hypoechoic, was diagnosed in the left common carotid, localized at the pain site, suggesting arteritis. However, the diagnosis was not clear. It evolved by thickening the common carotid on the right side, the innominate artery and the superior mesenteric. The wall has concentric circular lines similar to an onion. The affection is limited to the wall, as opposed to atherosclerosis that is projected to lumen.
More frequent in women (90%).
It usually starts before the fourth decade of life. Clinically,
it occurs due to claudication and absence of pulses in the upper limbs (subclavian affection),
visual alterations (retinal artery involvement),
as described by Takayasu in 1908,
and hypertension due to renal involvement in young patients.
The definitive diagnosis is made by biopsy of the arterial wall.
The ultrasound and Doppler diagnosis is made from the circumferential and concentric thickening of the arterial wall called "Macaroni sign".
The wall is hypoechoic,
with circular lines similar to an onion.
The affection is limited to the wall,
as opposed to atherosclerosis that is projected to lumen.

Fig. 10: A 32-year-old woman with arterial hypertension diagnosed with bilateral ostial renal artery stenosis and aortic wall thickening compatible with Takayasu disease. An evaluation is made with color Doppler of the neck vessels, detecting a thickening of the wall of the bilateral common carotid, larger on the left side.
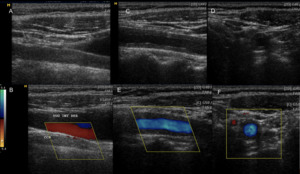
Fig. 11: A 32-year-old woman with arterial hypertension diagnosed with bilateral ostial renal artery stenosis and aortic wall thickening compatible with Takayasu disease. An evaluation is made with color Doppler of the neck vessels, detecting a thickening of the wall of the bilateral common carotid, larger on the left side.
- Postradiation arteritis: Numerous studies have shown a significant increase in the incidence of stenosis greater than 70%,
development of what seemed atheromatous plaques and increased intima media thickness in irradiated carotids with respect to the contralateral side and with control groups5.
The so-called post-radiation vasculopathy appears in 12 to 60% of the cases and not before 5 years of treatment.
Unlike cardiovascular disease,
severe disease was observed not only at the proximal level of ICA but also in CCA,
distal ICA and ECA,
with absence of atheromatous disease in other territories.

Fig. 12: Female patient, 46 years old with a history of left cervical irradiation. During a routine study, an ecodoppler was performed, observing left bulbar heterogeneous plaque causing a stenosis of 20-25% of the lumen and thickening of the median intimal thickness with respect to the contralateral thickness.
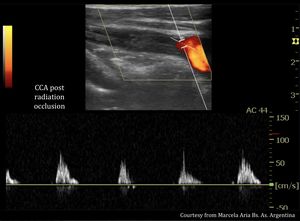
Fig. 13: 57-year-old male patient with a history of cervical irradiation due to Hodking lymphoma. The patient have a stroke. Color Doppler Ultrasound diagnosed occlusion of right primitive carotid artery.
4.D.
Carotidynia: Also called TIPIC syndrome (Transient Perivascular Inflammation of the Carotid Artery)10 is a very rare entity presented with unilateral neck pain,
and mostly is not suspected. It seems to be produced by the focal inflammation of the wall of the ICA by idiopathic,
infectious,
drug induced causes.
It has an autolimited evolution.
Duplex ultrasonography is the initial study recommended in the exploration of neck pain.
Focusing on the pain site,
a focal and not concentric thickened carotid wall is discovered,
often hypoechoic.
It can also be associated with intraluminal thrombus.
It may be accompanied by increased echogenicity of the pericarotid tissues 11,12. The changes observed are reversible.
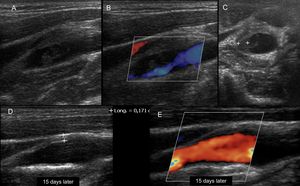
Fig. 14: 35-year-old patient with a history of Behcet's disease, presenting with unilateral cervical pain of 3 days of evolution. Ultrasound is performed with color Doppler demonstrating a focal thickening, asymmetric in the bulbar region of the internal carotid, with associated intraluminal thrombus. He underwent immunosuppressive treatment with corticosteroids and antibiotics. The picture resolves in 15 days to 1 month with resolution of parietal thickening and disappearance of the thrombus. It is interpreted as carotidynia or TIPIC syndrome.
4.E.
Fibromuscular dysplasia (FMD): is an uncommon vascular disease that affects the arteries of the body and is more commonly seen in women.
It affects medium-sized arteries.
The most commonly affected areas are the renal, carotid and vertebral arteries.
In FMD,
fibrous tissue and webs develop in the artery wall and can lead to narrowing of the arteries.
Patients with FMD can also develop bulging of the artery wall (aneurysms) or tears (dissections) of arteries and can have very twisty (tortuous) arteries.
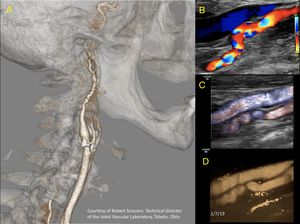
Fig. 15: A 35-year-old female patient with fibromuscular dysplasia of the internal carotid artery. The string of beds sign is observed. Marked tortuosity in the postbulb sector of the artery. A. 3D reconstruction angioCT B. Color Doppler. C. Dynamic flow. D. Microvasculature application
Courtesy of Bob Scissons from Toledo. Ohio. USA
There are two types of FMD8: multifocal and focal.
Multifocal FMD is by far the more common type (90%) of FMD and the hallmark sign is the ‘string of beads’ appearance of the artery,
which is widely recognized as a sign of FMD.
This occurs when areas of artery narrowing due to fibrous tissue and webs alternate with areas of artery enlargement or dilation.
Meanwhile,
focal FMD,
which is much less common,
usually consists of a single,
smoother narrowing in an artery,
with an intraluminal incomplete septum commonly affecting the posterolateral wall of the proximal ICA, also called ¨arterial web¨9.
The focal type is more common among young people.
Duplex ultrasound can identified beading,
turbulent blood flow,
higher velocities,
and tortuosity. The ¨S curve¨ is a distinct morphological pattern in the mid-distal ICA.
While it may not be specific to FMD,
its presence in individuals <70 years old should alert the clinician to the possibility that FMD is present7.
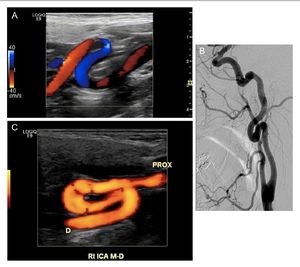
Fig. 16: Examples of S-curve morphologies from three different patients. Taken from Sethi, S.S., Olin, J.W. et al. The S curve: A novel morphological finding in the internal carotid artery in patients with fibromuscular dysplasia. Vascular Medicine, 2014, 19(5), 356–362.
References: Sethi, S.S., Olin, J.W. et al. The S curve: A novel morphological finding in the internal carotid artery in patients with fibromuscular dysplasia. Vascular Medicine, 2014, 19(5), 356–362.
4.F.
Aneurysm: is a focal dilatation of an artery that involves the three parietal layers.
They can be saccular or fusiform.
They are rare and occur more frequently in men,
beyond the sixth decade of life and associated with atherosclerosis.
They can be of inflammatory origin.
They most commonly involve the common carotid and the carotid bifurcation.
It is proposed that an increase in diameter greater than 50% with respect to the previous segment,
with intact walls,
is pathognomonic.
In doubtful cases,
it is useful to evaluate the maximum diameters and compare with the contralateral segments.
Clinically,
they present as painless pulsating masses.
Exceptionally,
they are associated with AIT-Stroke and compressive symptoms of cranial nerves.
The rupture is rare.
In ultrasound,
they are presented as focal dilatations,
with turbulent and swirling flow inside that can produce in color Doppler the sign of yin-yang. With spectral Doppler,
there is a decrease in intraaneurysmal velocities and turbulent and alternating flows.
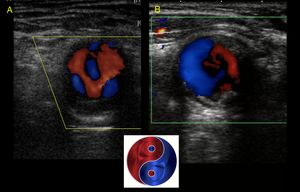
Fig. 17: Sign of Yin Yang in carotid aneurysms
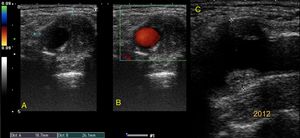
Fig. 18: Anurism of the distal common carotid artery in a 67-year-old male patient. Dilation greater than 50% of the previous segment and mural thrombus inside the lumen is observed.
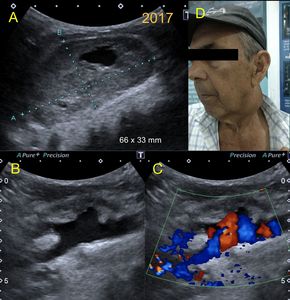
Fig. 19: Same patient as in figure 18, seen again 5 years later. There is a marked increase in the size of the aneurysm that is already known, with a large mural thrombus and deviation of the arterial flow towards the aneurysm lumen as if it were saccular. No clear limits of the aneurysm are observed. Complication is suspected. Continue in Figure 20.
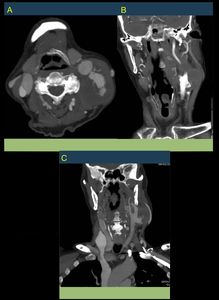
Fig. 20: Same patient of figures 18 and 19. Aneurysm of the Left Distal Common Carotid artery, with signs of complication. AngioCT is performed visualizing contrast leakage to adjacent tissues as signs of rupture.
4.G.
Pseudoaneurysm: is defined by the loss of integrity of the three layers of the arterial wall. The lesion of the arterial wall originates a blood extravasation which is contained by the soft tissues and compresed thrombus.
This generate a perivascular cavity,
with a false wall,
which can be partially thrombosed.
It communicate with arterial lumen through a neck.
Typically the flow in the neck is bidireccional,
¨to and fro¨,
with high velocities.
The most common origin of pseudoaneurysms is traumatic or iatrogenic,
secondary to a penetrating injury. It can also be a complication of dissections,
vasculitis,
fibromuscular dysplasia and phospholipid syndromes; finally they can be presented in endarterectomies or at bypass anastomosis.
Ultrasonographic and Doppler signs depend on the size of the pseudoaneurysm,
the neck and the degree of thrombosis present in its lumen.
The flow within the cavity is turbulent and swirling,
similar to aneurysms,
observing the sign of yin-yang in Color Doppler.
The spectral Doppler will show low speeds and turbulence.
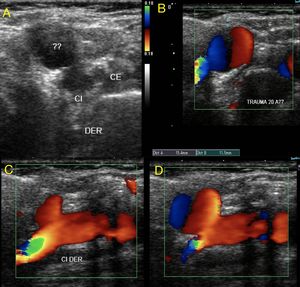
Fig. 21: Young male of 19 years with a history of closed trauma in the cervical region. Pseudoaneurysm of the internal carotid artery is observed. The outflow of arterial light into the peripheral tissue is identified. The leak is contained by the adjacent tissues. A wide neck is observed.
Fig. 22: Pseudoaneurysm of the ICA. It is the same case as in Figure 21.
A fissure in the arterial wall is observed through which flow is observed towards the false cavity or pseudoaneurysm.
4.H.
Arteriovenous fistula (AVF): It is a communication between an artery and a vein,
which in the topography of the neck would correspond most frequently to the carotid arterial system,
and the Jugular veins.
The mechanism by which it originates can be traumatic -blunt or penetrating-,
or iatrogenic -postcatheterism or postpunctions-.
Clinically they usually present with thrills and/or tinnitus due to the hyperflow generated in the communication due to the passage of blood from a high to a low pressure system.
There are also tortuosities and venous dilatations and edema generated in the venous system overload.
With Color Doppler the AVF are detected by the presence of color mosaic or aliasing and turbulence.
In the spectral analysis,
they show high velocities.
The afferent artery presents high velocity flows and decreased resistance and the efferent vein becomes pulsatile and can dilate identifying varices in infrequent territories.
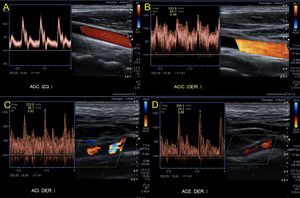
Fig. 23: A 27-year-old male patient self-inflicted with a knife wound on his neck. 1 month later, he attends by tinnitus and fremito. Increased velocities are observed, and turbulence in the spectra of the common, internal and external carotids of the right side (B, C and D). Continue on figure 24.
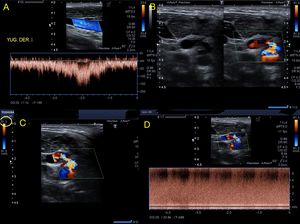
Fig. 24: A 27-year-old male patient self-inflicted with a knife wound on his neck. 1 month later, he attends by tinnitus and fremito. Increased velocities are observed, and turbulence in the spectra of the common, internal and external carotids of the right side. Pulsatile jugular venous flow is observed (A). The presence of an arteriovenous communication between the distal common carotid and the internal jugular vein of post-traumatic origin is confirmed (B and C). In this place, aliasing, turbulence, high speeds are observed (D). Continue in figure 25.
Fig. 25: Video that correspond to the same case describe in previous figures (23,24), showing the distal right common carotid and the internal jugular vein in cross section with a communication between them, with turbulent color Doppler flow and with mosaic or aliasing. The exact location of the lesion can be specified.
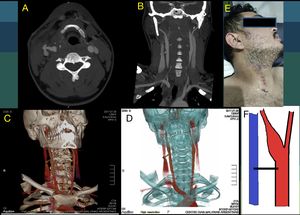
Fig. 26: This is a continuation of figures 23, 24 and 25. A 27-year-old male patient self-inflicted with a knife wound on his neck. 1 month later, he attends by tinnitus and fremito. Increased velocities are observed, and turbulence in the spectra of the common, internal and external carotids of the right side. Angioct scan is performed to confirm the finding.
4.I.
Dissection: A dissection is caused by a tear or disruption of an inner layer of the artery.
The blood flow dissects the layers,
and the intima is lifted from the artery wall.
This can generate a flap,
which divides the true light from the false one.
Sometimes,
the dissection is originated in a small bleeding inside the wall,
that generates a parietal hematoma that can push the intima towards the true lumen,
collapsing and occluding it.
The flap is not form in these cases.
In the Carotid arteries,
there are two types of dissections2.
- Primary dissections: Internal carotid artery (ICA) dissections typically occur just beyond the carotid bulb.
Dissections of the intracranial portion are much less common.
They clinically present in young individuals (< 50 years),
previously healthy,
usually with a headache and have nonspecific neurological symptoms,
only a sensory or motor deficit.
The dissection is spontaneous or posttrauma (rapid movements of the head).
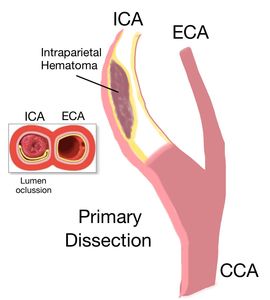
Fig. 27: Primary dissection of the Internal Carotid artery: It is originated in an intramural blood clot or a parietal hematoma that can push the intima towards the true light, collapsing and occluding it. The flap is not form in these cases.
This type of dissection of ICA is one of an intramural hematoma or thrombus.
If the size and volume of the blood clot is large enough,
the artery occludes.
If the size of the clot is intermediate, then the lesion causes a stenosis.
It is less common to see the double lumen with a separating intimal flap.
The intramural hematoma is hypoechoic and hard to perceive.
The Doppler findings are variable.
In the absence of a significant obstruction,
the signals can be normal.
When a large parietal hematoma compress the light,
produce a progressive cephalic narrowing,
with a duck's beak shape, a characteristic feature in angiography,
which can also be visualized in ultrasound.
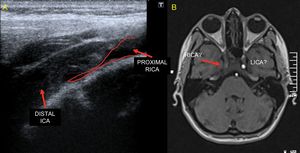
Fig. 28: Primary dissection of the ICA. When a large parietal hematoma compress the light, produce a progressive narrowing towards the distal, with the shape of a duck's bill (in red), a characteristic feature in angiography, but which can also be visualized with ultrasound. Continues on figure 29 (VIDEO) and 30.
Fig. 29: Continues from the case shown in the figure 28. Primary dissection of the ICA. Video showing first in transverse and then in longitudinal the ultrasound findings. When a large parietal hematoma compress the light, produce a progressive narrowing towards the distal, with the shape of a duck's bill, a characteristic feature in angiography, but which can also be visualized with ultrasound.Continues on figure 30.
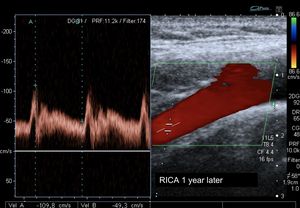
Fig. 30: resolution of the case shown in figures 28 and 29. Primary dissection of the carotid artery. Here we have an image of the same carotid 1 year after. The lumen is totally patent. The carotid artery has been recanalized. The parietal hematoma has been resolved and the intima back is attached to the other layers of the wall. Only a few mild neurological sequelae have been left.
- Secondary dissections: These dissections extend into the neck arteries from a primary dissection arising from the ascending aorta ‘‘type A’’. This is typically seen in older patients.
The symptoms are acute chest pain,
radiating to the back.
The extension of the dissection into the neck arteries is rarely symptomatic,
probably because the dissecting lumen re-enters the lumen at variable locations in the common or,
less often,
the ICA.
Neurologic symptoms are rare. Gray-scale imaging shows the typical luminal flap.
Doppler waveforms are altered.
If there is a site of re-entry,
forward blood flow is mainly seen.
If one of the lumens (the false lumen) does not re-enter the carotid lumen,
then an alternating systolic-diastolic waveform is seen in that lumen.
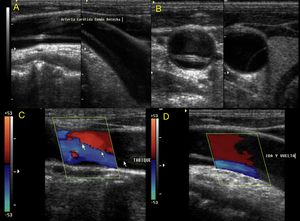
Fig. 31: Secondary dissection of the carotid (Common carotid): it affects the supra-aortic trunks, since in reality it is a type A dissection of the Aorta extended to the branches. It is usually displayed with the presence of flaps and flows from different directions on each side of the flap.
4.J.
Embolism: The embolus are thrombus that are usually originated in the left cardiac cavities.
They travel through the arterial circulation and can impact especially in areas of bifurcation,
abruptly occluding the lumen.
The size will determinate the caliber of the artery that they will occlude.
They can recanalize,
although they can leave neurological sequelae.
Ultrasound can show the material inside the artery fitted or not in the bifurcation.
It can produce an occlusion,
observing the absence of flow by color Doppler and preocclusive flows in the proximal sectors.
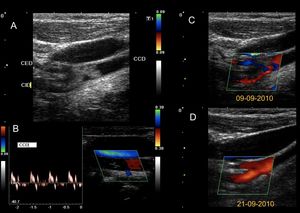
Fig. 32: 7 year old boy who suffers a stroke. He has a history of cardiac surgery for a single ventricle at birth. An echogenic material embedded in the carotid bifurcation compatible with embolism (A) is identified. The common carotid shows preobstructive flows (B). The embolism does not totally occlude the light, and allows to pass a small flow that is visualized with color Doppler (C). The patient is anticoagulated and 10 days later recanalizes the arterial light completely (D). However, it remains with severe ischemic neurological sequelae. It continues on figure 33.

Fig. 33: Continues from figure 32. 7 year old boy who suffers a stroke. He has a history of cardiac surgery for a single ventricle at birth. A carotid embolism is diagnosed by Ultrasound. Here are the most representative images of the AngioCT scan with 3D reconstruction at the time of the stroke, showing the absence of flow in the right common and interna carotid arteries. Not showing the cause.
4.K.
Carotid body tumors: Carotid Body Tumors (CBT) are typically benign,
slow-growing neoplasms.
They arise from the paraganglion cells located in the adventitia of the carotid body.
They represent 60-70% of paragangliomas of the head and neck.
Patients are often asymptomatic. Characteristically,
CBT can be detected by ultrasound as an ovoid hypoechoic mass,
solid,
with defined edges and hypervascularized with Color Doppler.
It is located in the carotid bifurcation,
separating the internal carotid from the external one,
opening the carotid bifurcation angle.
This has been described as the Lyre sign in angiography but we propose to call this particular disposition the “Atlas sign” in ultrasound.
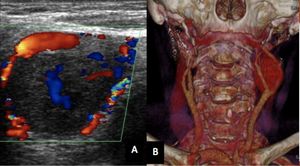
Fig. 34: Carotid body tumors can be detected by ultrasound as an ovoid hypo-echoic mass, solid, with defined edges and hyper-vascularized with Color Doppler. They are located in the carotid bifurcation, separating the internal carotid from the external one, opening the carotid bifurcation angle. This has been described as the Lyre sign in angiography but no sign was described in the ultrasound literature. We propose to call this particular disposition the “Atlas sign”. See next image
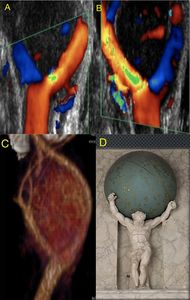
Fig. 35: Carotid body tumors can be detected by ultrasound as an ovoid hypo-echoic mass, solid, with defined edges and hyper-vascularized with Color Doppler. They are located in the carotid bifurcation, separating the internal carotid from the external one, opening the carotid bifurcation angle. This has been described as the Lyre sign in angiography but no sign was described in the ultrasound literature. We propose to call this particular disposition the “Atlas sign”.
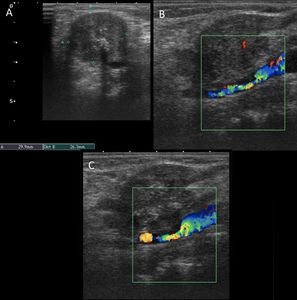
Fig. 36: Tumor invasion of the arterial wall of the internal carotid due to laryngeal tumor. A heterogeneous mass is observed in intimate contact with the ICA. The carotid wall in this sector shows irregularity and even some unusual material that projects slightly towards the light is observed. These findings are signs of tumor invasion due to contiguity.















, 356–362. References: Sethi, S.S., Olin, J.W. et al. The S curve: A novel morphological finding in the internal carotid artery in patients with fibromuscular dysplasia. Vascular Medicine, 2014, 19(5), 356–362.")





. Continue on figure 24.")
. The presence of an arteriovenous communication between the distal common carotid and the internal jugular vein of post-traumatic origin is confirmed (B and C). In this place, aliasing, turbulence, high speeds are observed (D). Continue in figure 25.")


, a characteristic feature in angiography, but which can also be visualized with ultrasound. Continues on figure 29 (VIDEO) and 30.")

: it affects the supra-aortic trunks, since in reality it is a type A dissection of the Aorta extended to the branches. It is usually displayed with the presence of flaps and flows from different directions on each side of the flap.")
 is identified. The common carotid shows preobstructive flows (B). The embolism does not totally occlude the light, and allows to pass a small flow that is visualized with color Doppler (C). The patient is anticoagulated and 10 days later recanalizes the arterial light completely (D). However, it remains with severe ischemic neurological sequelae. It continues on figure 33.")



