Type:
Educational Exhibit
Keywords:
Abdomen, Gastrointestinal tract, Oncology, CT, Diagnostic procedure, Neoplasia, Lymphoma
Authors:
M. LETURIA ETXEBERRIA1, A. Serdio2, M. Gredilla3, J. Elejondo Oddo4, K. Biurrun Mancisidor3; 1San Sebastian, Gipuzkoa/ES, 2Donostia - San Sebastián/ES, 3DONOSTIA/ES, 4San Sebastián/ES
DOI:
10.26044/ecr2019/C-1347
Background
a.
INTRODUCTION
Gastric cancer is the 6th most frequent malignancy in Europe and constitutes the 2nd most common carcinoma involving the gastrointestinal (GI) tract,
after colorectal carcinoma.
It is considered the 4th most common cause of cancer-related death.
Delayed detection is usual,
with the disease being disseminated in more than a half of the patients.
In fact,
approximately 60% of all present with unresectable disease.
As a consequence,
gastric cancer has a poor long-term clinical outcome,
with five-year survival rates varying from 10% to 30% in Europe.
Because final prognosis of the disease is related to parietal and adjacent structures invasion grade,
early diagnosis has demonstrated to be crucial in terms of improving survival rates of gastric cancer.
b.
CLASSIFICATION OF GASTRIC CANCER
1) BENIGN GASTRIC TUMOURS:
- Non-Neoplastic: hyperplastic polyps,
fundic gland polyps,
inflammatory fibroid polyp,
duplication cysts,
gastric heterotopic pancreas.
- Neoplastic: adenomas,
haemangiomas,
gastrointestinal stromal tumours,
lipomas,
leiomyomas,
schwannomas,
plexiform fibromyxomas.
2) MALIGNANT GASTRIC TUMOURS:
- Primary or Gastric Cancer: this review focuses on primary gastric cancer,
which histologically consists of:
− Adenocarcinoma (90-95%)
− Lymphoma (3-5%)
− GIST (2-3%)
− Carcinoid (gastric neuroendocrine) tumour
|
- Secondary malignancies: metastases or secondary neoplastic infiltration by contiguous spread.
c.
IMAGING MODALITIES FOR GASTRIC ASSESSMENT
Although histopathological diagnosis is required to declare definitive diagnosis of gastric cancer,
which is usually carried out by gastroscopic biopsy,
several imaging techniques are performed on a daily basis for gastric evaluation.
- Conventional baritated studies. In these, positive intraluminal contrast agents (e.g.
barium) are used to identify gastric wall alterations.
Nevertheless,
these techniques are decreasingly used.
- Endoscopic Ultrasound (EUS).
This minimally invasive modality enables transmural as well as locorregional lympadenopathies evaluation.
In addition,
biopsies could be performed,
which are specially useful for submucous tumours (such as GISTs),
as these can be easily ignored in conventional gastrosopy.
- Computed Tomography (CT). Modality of choice for diagnosis,
staging and post-treatment control.
Optimal gastric distension is a requirement for adequate gastric wall asessment; otherwise,
due to suboptimal distension,
false images of pseudotumours could be seen.
The CT protocol for suspected gastric cancer is summarised in Fig. 2 .
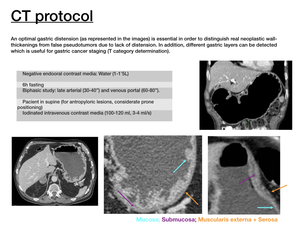
Fig. 2
- Magnetic Resonance (MR).
Used as an alternative when CT can not be used.
- Positron Emission Tomography (PET) is mainly used for distant metastases detection.
- Octreotide scan (somatostatin receptor scintigraphy).
As carcinoid tumoral cells express somatostatin receptors on their surface,
this modality is used for evaluation of carcinoid tumours.

