ECR 2019 / C-1462
MRI of Tumors in Pregnancy
Congress:
ECR 2019
Poster Number:
C-1462
Type:
Educational Exhibit
Keywords:
Obstetrics (Pregnancy / birth / postnatal period), Oncology, MR, Diagnostic procedure, Cancer, Foetus
Authors:
N. Kinger1, P. Mittal2; 1Atlanta, GA/US, 2Decatur, GA/US
DOI:
10.26044/ecr2019/C-1462

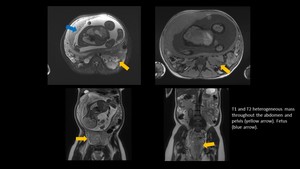
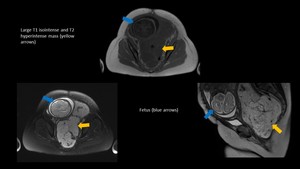
Fig. 1:
Plexiform Neurofibroma

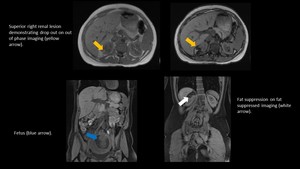
Fig. 2:
Angiomyolipoma

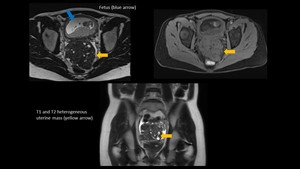
Fig. 3:
Uterine Fibroid

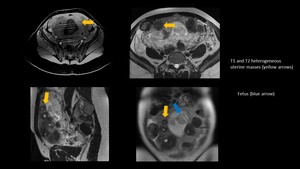
Fig. 4:
Extensive Uterine Fibroids

Fig. 5:
Cystic Degeneration of Intramural Fibroid

Fig. 6:
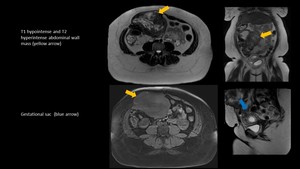
Desmoid Tumor

Fig. 7

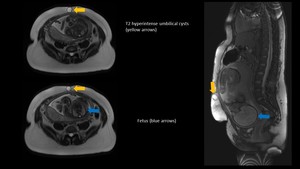
Fig. 8:
Umbilical Cyst

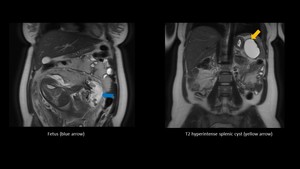
Fig. 9:
Splenic Pseudocyst

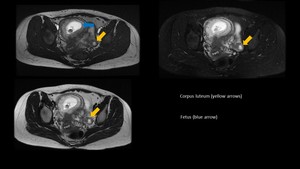
Fig. 10:
Corpus Luteum

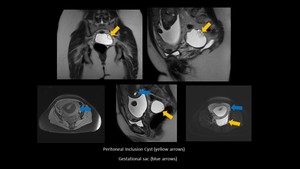
Fig. 11:
Peritoneal Inclusion Cyst

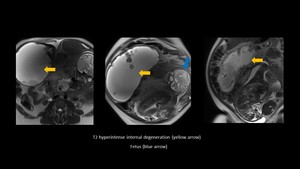
Fig. 12:
Hepatic Adenoma

Fig. 13:
Ovarian Mature Cystic Teratoma

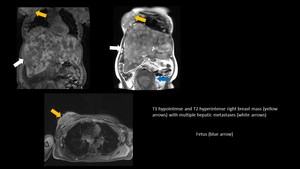
Fig. 14:
Breast Cancer

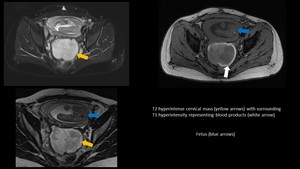
Fig. 15:
Cervical Adenocarcinoma

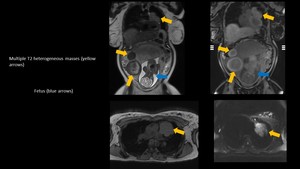
Fig. 16:
Epithelioid Neoplasm

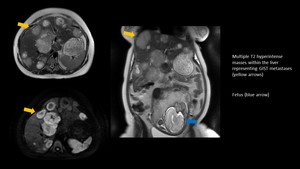
Fig. 17:
Gastrointestinal Stromal Tumor

Fig. 18:
Ovarian STUMP Tumor

Fig. 19:
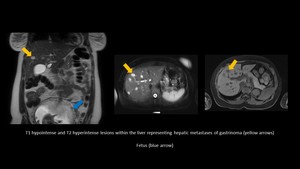
Gastrinoma

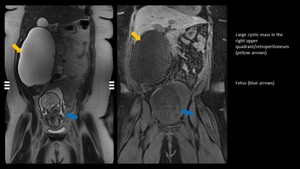
Fig. 20:
Cystic Mucinous Adenocarcinoma of the Retroperitoneum