ECR 2019 / C-1510
Imaging of thoracic-abdominal complications after cancer therapy
Congress:
ECR 2019
Poster Number:
C-1510
Type:
Educational Exhibit
Keywords:
Radiation effects, Complications, Chemotherapy, CT, Oncology, Thorax, Abdomen, Multidisciplinary cancer care, Toxicity
Authors:
J. Hu, A. Campagnola, M. C. Ambrosetti, G. A. Zamboni, G. Mansueto; Verona/IT
DOI:
10.26044/ecr2019/C-1510
. Adapted from: CT findings of chemotherapy-induced toxicity, Torrisi et al., Radiology. 2011;258(1): 41-56. References: CT findings of chemotherapy-induced toxicity, Torrisi et al., Radiology. 2011;258(1): 41-56.")
Table 1:
List of the most frequent side effects of chemotherapy, classic and "target",...

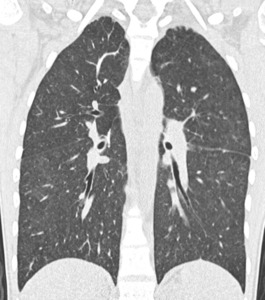
Fig. 1:
24-year-old Patient with Hodgkin's sclero-nodular lymphoma sc II.
NSIP CT...

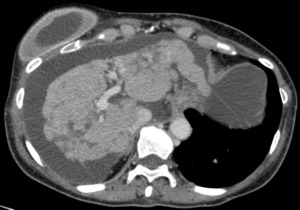
Fig. 2:
67-year-old Patient affected by breast adenocarcinoma, treated with multiple...
. CT shows hepatic sinusoidal occlusive syndrome.")
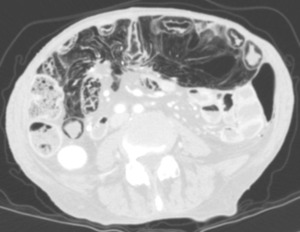
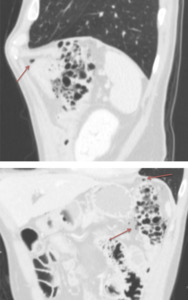
Fig. 3:
64-year-old Patient affected by uterine carcinoma, IV stage FIGO, undergoing...
.
Routine staging CT shows important intestinal pneumatosis, in an asymptomatic subject.")
Fig. 4:
An 80-year-old Patient with advanced adenocarcinoma of sigma and pulmonary and...
 in the peritoneal cavity, compatible with perforation.")
Fig. 5:
59-year-old Patient with T lymphoma treated with Cyclophosphamide, Doxorubicin...
 affected by uterine carcinoma, IV stage FIGO, undergoing radical surgery and chemotherapy (paclitaxel + carboplatin). CT shows also the presence of a floating thrombus in thoracic aorta.")
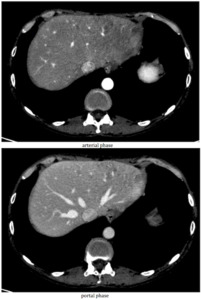
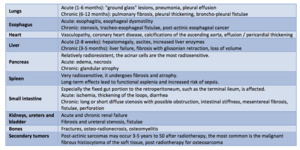
Fig. 6:
The same 64-year-old Patient (in figure 2) affected by uterine carcinoma, IV...

Fig. 7:
84-year-old Patient affected by renal cell carcinoma with a radiotreated...

Table 2:
Main post-radiotherapy complications divided by irradiated organ.