The evolution of imaging techniques and their increased use in clinical practice have led to a higher detection rate of UIAs.
Until 1995,
surgical clipping of the aneurysm was the only approach available.
Nowadays, the treatment of UIAs remains complex.
While for ruptured intracranial aneurysms the management are well defined by several trials,
for asymptomatic UIAs the best option is still uncertain.
PATHOPHISIOLOGY
An aneurysm is an abnormal dilatation of an artery,
arising from focal hemodynamic stress,
inflammation,
and genetic factors.
Mechanism of formation.
- Aneurysm formation begins with hemodynamic stress,
which typically occurs at arterial branch points or abrupt arterial angles,
where stress triggers endothelial dysfunction.
- Endothelial dysfunction leads to a loss of endothelian nitric oxide synthase production and increased expression of inflammatory mediators and cytokines.
- Arterial inflammation leads to apoptosis of smooth muscle cells and matrix metalloproteinase- mediated erosion of the extracellular matrix.
Inflammation in aneurysm formation has two primary components :
- Smooth muscle cell migration and transformation.
Normally,
smooth muscle cells are concentrated in the media and are the predominant matrix-synthesizing cells of the arterial wall.
During aneurysm formation,
smooth muscle cells migrate into the intima in response to endothelial injury and multiply,
leading to myointimal hyperplasia .
Under these conditions,
smooth muscle cells undergo phenotypic transformation into dissociated,
spider-like cells with impaired collagen-synthesis capacity and contractility .
Late in aneurysm formation,
a loss of smooth muscle cells occurs in the aneurysm wall,
along with thinning of the media .
- Macrophage involvement.
Macrophage activation and infiltration of the artery wall occurs in response to inflammatory mediators.
Macrophages release inflammatory cytokines and matrix metalloproteinases,
which digest the artery wall extracellular matrix.
Weakening of the extracellular matrix in this manner contributes to aneurysm progression.
Macrophage infiltration is strongly associated with aneurysm rupture.
Myeloperoxidase expression is also increased,
and is a marker for aneurysm rupture .

Fig. 1: PATHOPHISIOLOGY OF THE UIA
References: Nohra Chalouhi, MD; Brian L. Hoh, MD; David Hasan, MD. 2013. Review of Cerebral Aneurysm Formation, Growth, and Rupture. Stroke. 44:3613-3622.
Morphological features: Multiple lobes apears in 9% and a daughter sac is found in 16% of unruptured aneurysms.
Site distribution(unruptured aneurysms in patients with no prior history of SAH).
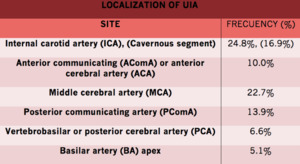
Fig. 2
References: Mark R. Harrigan and John P. Deveikis. 2018. Handbook of Cerebrovascular Disease and Neurointerventional Technique. Springer International Publishing AG. ISBN 978-3-319-66777-5.
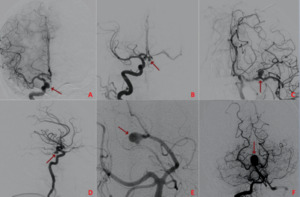
Fig. 3: Digital subtraction angiography (DSA) shows tipical localization of aneurysm: ICA (A), AcomA (B), MCA (C), PComA (D), PCA (E) and BA apex (F)
Risk factors for aneurysm formation: female sex,
cigarette smoking,
hypertension,
a family history of cerebrovascular disease and postmenopausal
state.
PREVALENCE
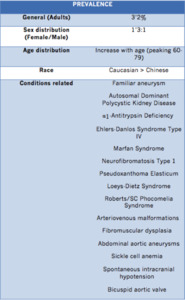
Fig. 4
References: Mark R. Harrigan and John P. Deveikis. 2018. Handbook of Cerebrovascular Disease and Neurointerventional Technique. Springer International Publishing AG. ISBN 978-3-319-66777-5
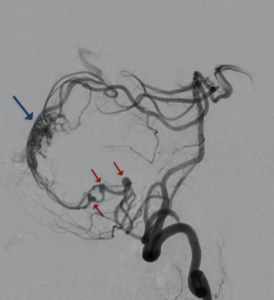
Fig. 5: Angiography reveals an AVM of the region of the torcula. Three distal flow-related aneurysms are seen to originate from the feeding PICA of the AVM nidus
Unruptured aneurysms have been diagnosed at an increasing rate in recent years,
probably as
a result of the improving quality and growing use of noninvasive imaging techniques.
NATURAL HISTORY
The natural history of unruptured intracranial aneurysms has come into focus with the publication of several large-scale prospective studies: International Study of Unruptured Intracraneal Aneurysm (ISUIA),
The Unruptured Cerebral Aneurysm Study of Japan (UCAS),
and Small Unruptured Intracranial Aneurysm Verification Study (SUAVe).
A famous study from Finland of 142 patients with a median follow-up of 21 years reported an overall average annual rupture risk of 1.1%.

Fig. 6
References: ISUIA, UCAs, SUAVe trials and Comprehensive Observational Cohort Study in Finland.
In a recent article,
Greving et al.
proposed a practical risk score called PHASES score.
It is used to predict a patient’s risk of aneurysmal rupture based on population (geographical location),
hypertension,
age,
size of aneurysm,
earlier subarachnoid hemorrhage from another aneurysm,
and site of aneurysm.
These predictors were selected based on a systematic review of and pooled analysis from 8382 participants in 6 prospective cohort studies with subarachnoid hemorrhage as outcome.
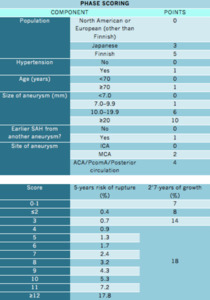
Fig. 7
References: Greving JP. El al. 2014 Development of the PHASES score for prediction of risk of rupture of intracranial aneurysms: a pooled analysis of six prospective cohort studies. Lancet Neurol. 13(1):59-66.
