ECR 2019 / C-1893
Applying CT/MRI LI-RADS v2018 imaging features in interpreting liver MRI of patients at risk of HCC: a simplified approach for the juniors
Congress:
ECR 2019
Poster Number:
C-1893
Type:
Educational Exhibit
Keywords:
Multidisciplinary cancer care, Education and training, Education, Diagnostic procedure, MR, Liver, Abdomen
Authors:
M. T. El-Diasty1, M. Wazzan1, H. Sadec2, M. AbouRayan3, M. M. A. Rezk4, A. Abduljabbar1; 1Jeddah/SA, 2Alexandria /EG, 3Alexandria/EG, 4Cairo/EG
DOI:
10.26044/ecr2019/C-1893

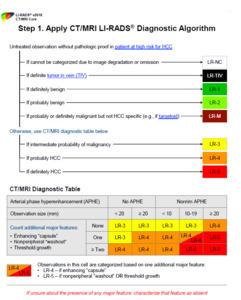
Fig. 13:
Step 1 of the LI-RADS algorithm is the designation of a preliminary LIRADS...

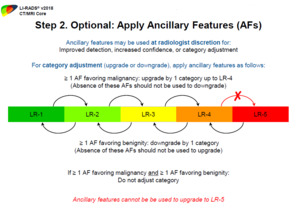
Fig. 14:
Step 2 of the algorithm is the optional application of ancillary features for...

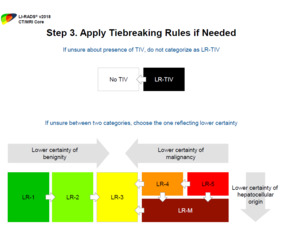
Fig. 15:
Step 3 is the application of tiebreaking rules in situations of diagnostic...

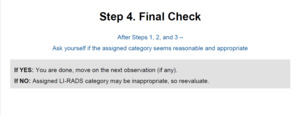
Fig. 16:
Step 4 is the final check to verify that the assigned category is reasonable...

Fig. 17:
Major changes in previous LI-RADS versions
 2017 Version of LI-RADS for CT and MR Imaging: An Update. Radiographics. 37(7): p. 1994-2017.")
Fig. 18:
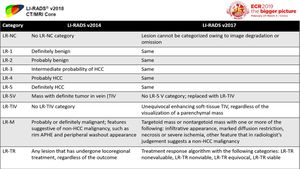
Comparison between LI-RADS 2014 & LI-RADS 2017
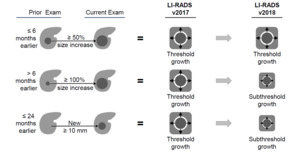
 are considered subthreshold growth in v2018 References: Reproduced from LI-RADS v2018 with permission from the American college of Radiology")
Fig. 19:
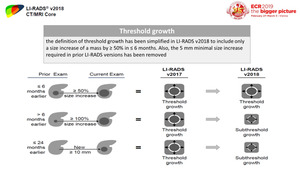
Change in threshold growth definition in LI-RADS v2018.
Two other definitions...

Fig. 20:
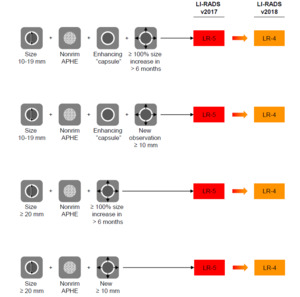
The impact of change in threshold growth definition on categorization of...
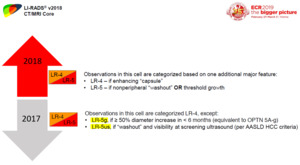
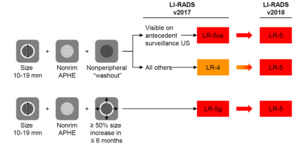
 on CT/MRI in addition to ≥ 50% increase in size in < 6 months, but without ‘‘washout’’ or ‘‘capsule’’. This category was originally introduced to facilitate translation to OPTN class 5 criteria—specifically OPTN 5A-g. In LI-RADS v2018, 10-19 mm observations with APHE and threshold growth are now simply categorized LR-5, as the threshold growth definition is identical to that of OPTN.
The LR-5us category was previously applied to observations 10–19 mm in size with nonrim APHE, ‘‘washout’’ and visibility at antecedent screening ultrasound, in absence of either threshold growth or a ‘‘capsule’’. In LI-RADS v2018, the requirement for antecedent visibility on ultrasound has been removed, and a 10–19 mm observation with nonrim APHE and nonperipheral ‘‘washout’’ is categorized LR-5.")
Fig. 21:
Changes in LR-5 criteria between LI-RADS 2017 and LI-RADS 2018
The LR-5g...

Fig. 22:
The impact of change in LR-5 criteria in LI-RADS v2018

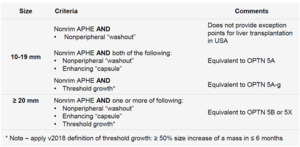
Fig. 23:
New LR-5 criteria in LI-RADS v2018
 References: Reproduced from LI-RADS v2018 with permission from the American college of Radiology")
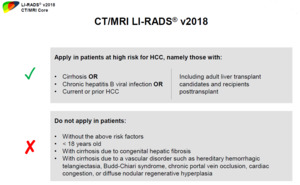
Fig. 24:
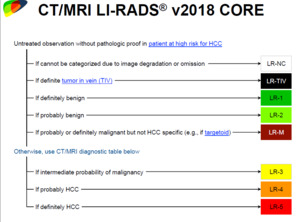
LI-RADS population (patients at risk of HCC)

Fig. 25:
LI-RADS diagnostic categories

Fig. 26:
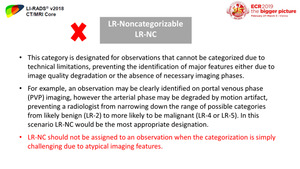
LR-NC category

Fig. 27:
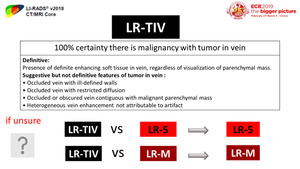
LR-TIV category

Fig. 28:
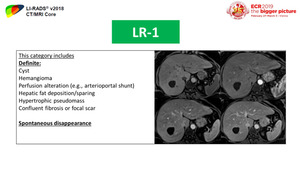
LR-1 category

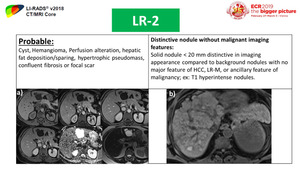
Fig. 29:
LR-2 category

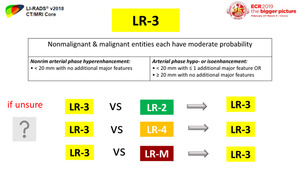
Fig. 30:
LR-3 category

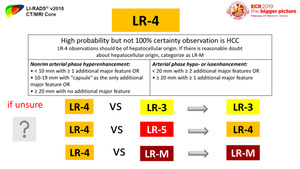
Fig. 31:
LR-4 category

Fig. 33:
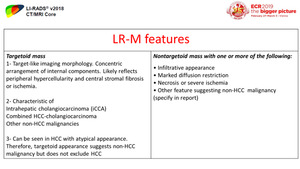
LR-M category

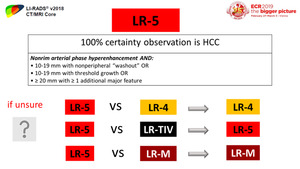
Fig. 32:
LR-5 category

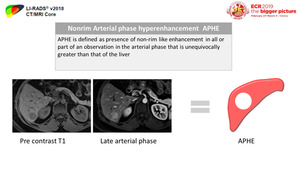
Fig. 34:
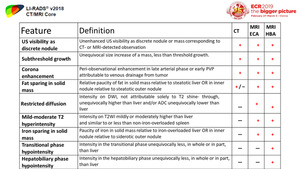
Definition of APHE

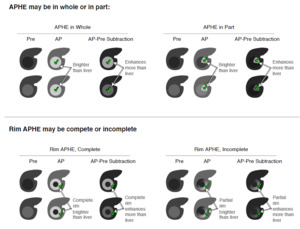
Fig. 35:
Difference between non-rim APHE and rim APHE

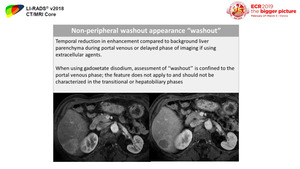
Fig. 36:
Definition of non-rim washout appearance "washout"

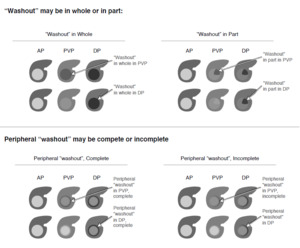
Fig. 37:
Difference between non-peripheral and peripheral washout

Fig. 38:
Patterns of APHE & "washout"

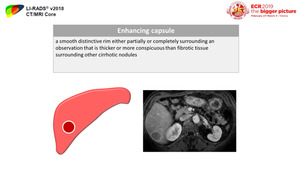
Fig. 39:
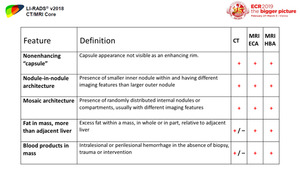
Definition of enhancing capsule appearance

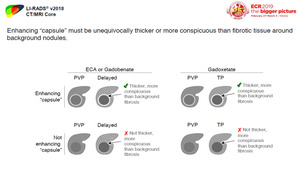
Fig. 40:
Capsule appearance with ECA, Gadobenate and Gadoxetate

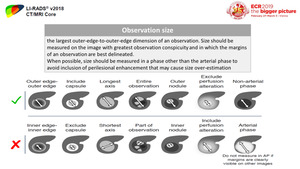
Fig. 41:
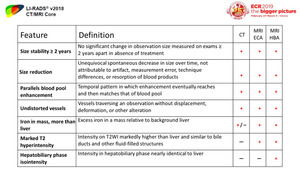
Definition of observation size and accurate measurements

Fig. 42:
Definition of threshold growth in LI-RADSv2018

Fig. 43:
LR-M features

Fig. 44:
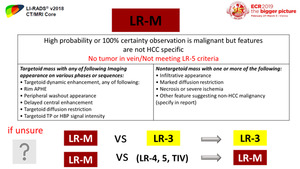
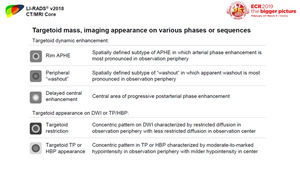
Imaging appearance of targetoid mass

Fig. 45:
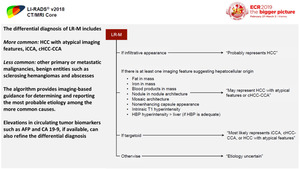
Differential diagnosis and algorithm for LR-M category

Fig. 46:
Ancillary features favoring malignancy in general not specific for HCC

Fig. 47:
Ancillary feature favoring HCC in particular

Fig. 48:
Ancillary features favoring benignity

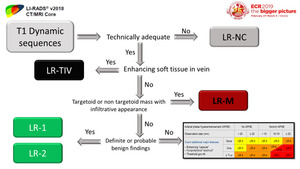
Fig. 49:
Interpreting approach, part 1

Fig. 50:
Interpreting approach part 2