Pcomm were visualized in 34 (63%) patients: in 18 patients - unilateral,
in 16 patients - bilateral.
Variant anatomy related to COW was found in 26 (48%) patients
The main COW variants were identified:
- Posterior ICA trifurcation in 13 (24%) patients
- ACA А1 segment hypoplasia in 5 (9%) patients
- V4 segment VA hypoplasia in 8 (15%) patients
Most frequently posterior ICA trifurcation was detected (13 patients – 24%).
This variant refers to the fetal brain blood supply type which remains in adulthood.
In this variant anterior and posterior cerebral blood flow derive from one stream from ICA due to the primary (fetal) Pcomm giving a rise to PCA.
Normal fetal Pcomm is reducing during the ontogenesis and replaced by normal Pcomm in adulthood according to the researchers reports [3]
Posterior ICA trifurcation had met in 2 types
- PCA on side of trifurcation derives from a fetal Pcomm and there is its P1 hypoplasia (8 patients) [figure 3A].
- Separation of fetal Pcomm from PCA and the presence of two separate arteries (5 patients) [figure 3B].
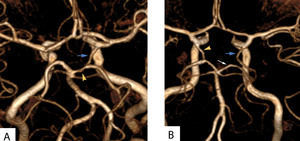
Fig. 3: M3D/TOF/SP/GP. A: Posterior trifurcation of left ICA is detected (blue arrow) with P1 segment PCA hypoplasia (yellow arrow). B: Posterior trifurcation of left ICA (blue arrow), separate ipsilateral PCA (wile arrow), contralateral Pcomm (yellow arrow).
References: Department of Radiology, MEDSI, Botkin hospital, Moscow
These types of ICA trifurcation were detected in 8 patients on the one side,
in 5 patients on the both sides.
In 4 cases (50%) unilateral posterior ICA trifurcation was combined with contralateral Pcomm visualization (<1.5 mm – in 3 patients,
> 1.5 mm- in 1 patient) [Table 2].
Table 2. Variants of ICA trifurcation with contralateral Pcomm combination
|
Variant of ICA trifurcation/Pcomm (n)
|
Pcomm<1,5 mm (n)
|
Pcomm>1,5 mm (n)
|
|
PCA and fPcomm connected (8)
|
1
|
-
|
|
PCA and fPcomm disconnected (5)
|
-
|
3
|
The blood flow MR signal estimation in posterior ICA trifurcation was not revealing a direct connection with the need for the collateral flow development.
The presence of contralateral Pcomm in posterior ICA trifurcation in 50% of cases could be associated with blood flow compensation in the other hemisphere in the intrauterine period or with the presence of fetal Pcomm on the other side
Frequency of other variants was substantially lower (ACA А1 segment hypoplasia in 5 (9%) patients and VA hypoplasia – in 8 (15%) patients).
In case of ACA and VA hypoplasia only one Pcomm was detected (ipsilateral in VA hypoplasia,
contralateral in ACA hypoplasia,
frequency demonstrated in table [table 3].
Table 3. VA and ACA hypoplasia with contralateral Pcomm combination
|
Variant/Pcomm (n)
|
Pcomm<1,5 mm (n)
|
Pcomm>1,5 mm (n)
|
|
side
|
side
|
|
Ipsi-
|
contr-
|
ipsi-
|
contr-
|
|
VA hypoplasia/aplasia (8)
|
3
|
-
|
5
|
-
|
|
A1 segment ACA hypoplasia (5)
|
-
|
4
|
-
|
-
|
This table demonstrates 100% compatibility of VA hypoplasia with ipsilateral Pcomm with predominance larger arteries,
80% compatibility of ACA hypoplasia with contralateral Pcomm [figure 4].

Fig. 4: Left A1 segment of ACA hypoplasia (white arrow) with contralateral Pcomm (yellow arrow) on the M3D/TOF/SP/GP is detected.
References: Department of Radiology, MEDSI, Botkin hospital, Moscow
Hypoplasia of the vertebral artery occurred in two types:
- Aplasia of the intracranial segment of VA and transition of VA to the posterior inferior cerebellar artery and the origin of OA from the opposite VA (3 patients) [figure 6A].
- Hypoplasia of the intracranial segment of VA which was traced throughout and formed BA by merging with the opposite VA (5 patients) [figure 5]
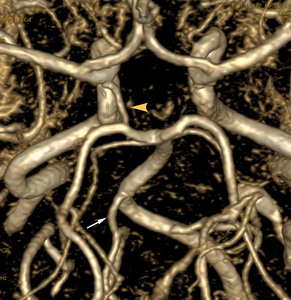
Fig. 5: Right VA hypoplasia (white arrow) with ipsilateral Pcomm (yellow arrow) on the M3D/TOF/SP/GP is detected.
References: Department of Radiology, MEDSI, Botkin hospital, Moscow
In 3 patients,
VA hypoplasia/aplasia was combined with posterior ICA trifurcation and fetal Pcomm type.
To simplify statistical processing patients with this combination of variants were assigned to the group with Pcomm > 1.5 mm [figure 6 A,
B].
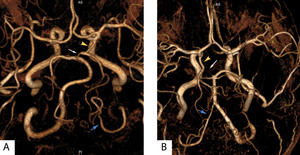
Fig. 6: M3D/TOF/SP/GP. A: left VA last segment aplasia (blue arrow) is detected added of posterior trifurcation of left ICA (yellow arrow) with P1 segment PCA hypoplasia (white arrow). B: Right VA aplasia (blue arrow) is detected added of posterior trifurcation of right ICA (yellow arrow) with severe P1 segment PCA hypoplasia (white arrow).
References: Department of Radiology, MEDSI, Botkin hospital, Moscow
In one female patient (34 yeas age) aplasia of the VA was defined and this was combined with the ipsilateral Pcomm of small diameter (< 1.5 mm) detected only on 2D.
In this patient cortical ischemic stroke of the occipital lobe was additionally revealed on the side of VA aplasia.
Obviously insufficient flow in PCA had contributed to stroke formation [figure 7 A,
B,
C].
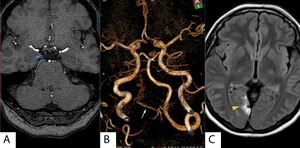
Fig. 7: A: Right Pcomm on axial M3D/TOF /SP/GP are detected in minimal diameter <1,5 mm (Blue arrow). B: Right VA aplasia (white arrow) is detected but there is no support of any Pcomms. C: Hight signal intensity from cortical ischemic stroke (yellow arrow) is detected on axial FLAIR.
References: Department of Radiology, MEDSI, Botkin hospital, Moscow
The other 28 (52%) patients had a normal closed COW.
Pcomm was not detected in 9 patients.
These patients were assigned to group 1 with arteries of very small diameter,
undetectable due to method limitations [figure 8].
Fig. 8: M3D/TOF /SP/GP. Normal anatomy of COW.
References: Department of Radiology, MEDSI, Botkin hospital, Moscow
Visualization of Pcomm was observed in 19 (67%) patients with normal COW.
The presence of Pcomm in patients with normal COW was distributed as sown in table [table 4].
Table 4.
Distribution of Pcomm visualization in patients with normal COW
|
Group 1 not defined
|
Group 2 < 1,5 mm
|
Group 3 > 1,5 mm
|
|
|
Unilateral
|
Bilateral
|
Unilateral
|
Bilateral
|
|
9
|
9
|
4
|
2
|
4
|
The table 4 shows the visualization of the MR-signal from the blood flow in the Pcomm in patients with a normal COW: in 13 patients Pcomm smaler diameter (group 2),
in 6 patients Pcomm larger diameter (group 3).
Diameter of Pcomm`s from group 3 visually were comparable to the diameter of the rest of the arteries of the cerebral circulation [figure 9 A,
B].
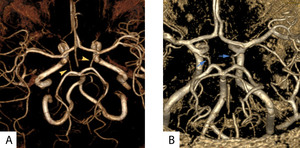
Fig. 9: Normal anatomy of COW is detected on M3D/TOF /SP/GP. A: Bilateral Pcomm`s of small diameter (yellow arrowes). B: Bilateral Pcomm`s of large diameter (blue arrowes).
References: Department of Radiology, MEDSI, Botkin hospital, Moscow
The fact detection in some cases of Pcomm diameter of which comparable to the diameter of the posterior cerebral arteries in normal COW,
as well as the fact that the hypoplasia of PCA in posterior ICA trifurcation could be appear in varying degrees,
allowed us to assume the possibility preservation of a fetal Pcomm in adulthood without any COW arteries hypoplasia (mainly PCA) [figure 10 A,
B,
C,
D].
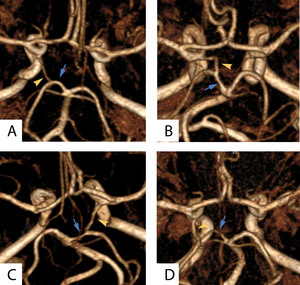
Fig. 10: M3D/TOF /SP/GP. This picture demonstrates cases of COW appearance gradation from a small Pcomm and large Pcomm (yellow arrowes) visualisation without any PCA (blue arrow) hypoplasia (A,B) toward posterior ICA trifurcation and fetal Pcomm (yellow arrow) visualisation with several degrees of PCA (blue arrow) hypoplasia (C,D).
References: Department of Radiology, MEDSI, Botkin hospital, Moscow
We also assume that the presence of developed Pcomm (more than 1.5 mm) and normal caliber of other COW arteries is a transitional form between the normal and fetal type of cerebral blood circulation.
And this is confirmed by the frequency of Pcomm in the 3rd group reflected in the table 4.

 with P1 segment PCA hypoplasia (yellow arrow). B: Posterior trifurcation of left ICA (blue arrow), separate ipsilateral PCA (wile arrow), contralateral Pcomm (yellow arrow). References: Department of Radiology, MEDSI, Botkin hospital, Moscow")
 with contralateral Pcomm (yellow arrow) on the M3D/TOF/SP/GP is detected.
References: Department of Radiology, MEDSI, Botkin hospital, Moscow")
 with ipsilateral Pcomm (yellow arrow) on the M3D/TOF/SP/GP is detected. References: Department of Radiology, MEDSI, Botkin hospital, Moscow")
 is detected added of posterior trifurcation of left ICA (yellow arrow) with P1 segment PCA hypoplasia (white arrow). B: Right VA aplasia (blue arrow) is detected added of posterior trifurcation of right ICA (yellow arrow) with severe P1 segment PCA hypoplasia (white arrow). References: Department of Radiology, MEDSI, Botkin hospital, Moscow")
. B: Right VA aplasia (white arrow) is detected but there is no support of any Pcomms. C: Hight signal intensity from cortical ischemic stroke (yellow arrow) is detected on axial FLAIR. References: Department of Radiology, MEDSI, Botkin hospital, Moscow")

 visualisation without any PCA (blue arrow) hypoplasia (A,B) toward posterior ICA trifurcation and fetal Pcomm (yellow arrow) visualisation with several degrees of PCA (blue arrow) hypoplasia (C,D). References: Department of Radiology, MEDSI, Botkin hospital, Moscow")