ECR 2019 / C-1959
A multidisciplinary review of clinical data exchange concerning ordering of CT angiograms in patients with suspected pulmonary embolism.
Congress:
ECR 2019
Poster Number:
C-1959
Type:
Scientific Exhibit
Keywords:
Management, Pulmonary vessels, Professional issues, CT-Angiography, Structured reporting, Efficacy studies, Statistics, Quality assurance, Epidemiology, Workforce
Authors:
M. Buk1, O. von Stackelberg2, E. Giannitsis2, L. Kihm2, H. U. Kauczor2, T. F. Weber2; 1Prague/CZ, 2Heidelberg/DE
DOI:
10.26044/ecr2019/C-1959

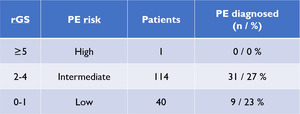
Table 2:
Actual PE findings according to the rGS-based risk stratification

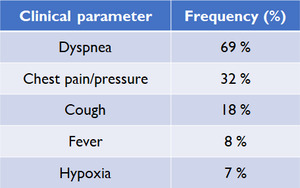
Table 3:
Important clinical parameters included in the rGS, yet they were not...

Table 4:
Other clinical parameters from the CTPA request forms, which are however not...