CT pulmonary angiography (CTPA) is the gold standard imaging technique for suspected pulmonary embolism (PE).
However,
it carries the burden of radiation exposure and the need for using an iodine-based intravenous contrast agent.
The aim of our study was to review if CTPA examinations were being correctly indicated in accordance with the ALARA principle and current diagnostic guidelines at the Department of Diagnostic and Interventional Radiology at the University Hospital in Heidelberg,
Germany.
For assessing the appropriateness of CTPA examinations,
the diagnostic algorithm from ESC Guidelines on Pulmonary Embolism from the year 2014 was used.[1] The decision,
according to these guidelines,
is made based on D-dimer value and clinical scoring system - simplified revised Geneva Score (rGS) for clinically stable patients,
or low-risk patients (see Figure 1).
The rGS (these guidelines use the simplified version) is calculated as a sum of specific clinical parameters (see Table 1).
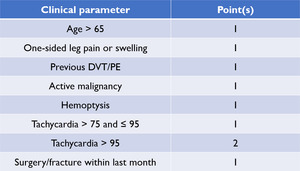
Table 1: Simplified revised Geneva Score clinical parameters overview.
References: Department of Diagnostic and Interventional Radiology, University Hospital Heidelberg, Germany
This rGS value further categorizes the patients based on either a dichotomized score or a 3-level score.
The dichotomized score differentiates between a low probability of PE (score < 3) and a high probability of PE (score ≥ 3),
which is what the diagnostic algorithm is based on.
The 3-level score differentiates between low,
intermediate and high risk of PE.
According to the study of Ceriani et al.
the incidence of PE is reported as follows: in the high-risk group up to 65%; in the intermediate-risk group up to 30% and in the low-risk group up to 10% of cases.[2]
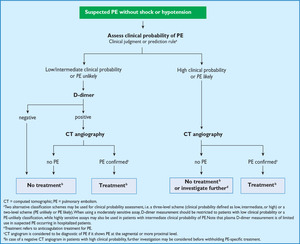
Fig. 1: Proposed diagnostic algorithm for patients with suspected non-high-risk PE (i.e. without shock and hypotension).
References: Eur Heart J. 2014 Nov 14;35(43):3033-69, 3069a-3069k.
As opposed to in clinically unstable patients or hospitalized patients (they are considered as unstable in all cases) it is always advised to perform CTPA to confirm or rule out suspected PE according to the guidelines (see Figure 2).
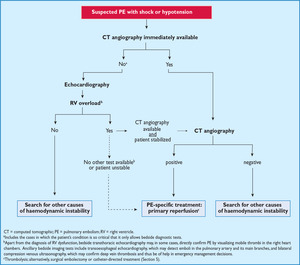
Fig. 2: Proposed diagnostic algorithm for patients with suspected high-risk PE, i.e. presenting with shock or hypotension.
References: Eur Heart J. 2014 Nov 14;35(43):3033-69, 3069a-3069k.
Aside from the evaluation of the clinical data,
there’s also the D-dimer value that plays an important role in the diagnostic algorithm.
The cutoff value is in this case set to 0.5 mg/l.[3] This value tends to yield false-positive results in hospitalized patients.[4] For this reason,
only outpatients were included in this study.
Positive D-dimer value (above cutoff) or rGS equal to or higher than 3 means that the CTPA is correctly indicated according to the guidelines.[1]
The objectives of this study were:
- To review the correctness of indication of CTPA examinations in clinically stable outpatients with suspected PE.
- To evaluate the availability of relevant clinical and laboratory data for the CTPA diagnostic guidelines from the Electronic Health Record (EHR) documentation within the Radiology Information System (RIS).
- To compare the actual PE findings percentages according to the clinical risk stratification based on data from previous studies.


. References: Eur Heart J. 2014 Nov 14;35(43):3033-69, 3069a-3069k.")
:3033-69, 3069a-3069k.")