ECR 2019 / C-1973
Tuberculosis: A Multiorgan Disease
Congress:
ECR 2019
Poster Number:
C-1973
Type:
Educational Exhibit
Keywords:
Lung, Abdomen, CNS, Conventional radiography, CT, MR, Computer Applications-General, Education, Localisation, Tissue characterisation, Kv imaging, Epidemiology
Authors:
A. R. Pugliesi1, M. I. Vögele1, W. Kersjes2, J. Degenkolb3, M. F. Ciolpan4, C. Utz1, A. Meixel5, M. A. Hesse1, M. R. Klein1; 1Ludwigsburg/DE, 2Bietigheim-Bissingen/DE, 3Gilching/DE, 4Karlsbad/DE, 5Heidelberg/DE
DOI:
10.26044/ecr2019/C-1973

Fig. 1:
Primary tuberculosis.

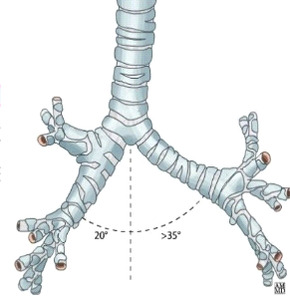
Fig. 2:
Bronchial Anatomy

Fig. 3:
PA CXR showing RT hilar enlargement secondary to lymphadenopathy, suggestive of...

Fig. 4:
PA CXR showing Pleural effusion in a 19 years old Patient affected by...

Fig. 5:
RT lateral CXR image showing Pleural effusion in a Patient affected by...

Fig. 6:
PA CXR showing an Adult affected by Tuberculosis.
.")
Fig. 7:
CT Image showing calcified lymph node commonly suggestive of Ranke complex...

Fig. 8:
PA CXR showing LT peripheral upper lung, small, ill-defined soft tissue nodule...

Fig. 9:
Tree-in-Bud in a patient with pulmonary tuberculosis.

Fig. 10:
Cavern links in a patient with pulmonary tuberculosis.

Fig. 11:
Pulmonary Tuberculosis, PA CXR.

Fig. 12:
CT scan showing parenchymal postprimary tuberculosis with the typical apical...

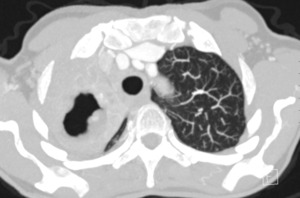
Fig. 13:
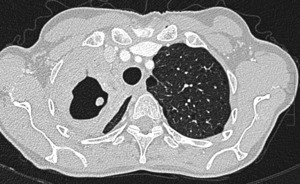
MIP axial Large TBC cavern in the CT-scan.

Fig. 14:
CT scan Miliary Tuberculosis. Innumerable, small, millet-seed sized nodules are...

Fig. 15:
Excavating tuberculosis, PA CXR.

Fig. 16:
Tuberculomas. PA CXR.

Fig. 17:
Scarring-fibrotic changes postprimary tuberculosis CT scan.

Fig. 18:
Scarring-fibrotic changes postprimary tuberculosis CT scan.

Fig. 19:
Patient affected by Tuberculosis.

Fig. 20:
Patient affected by Tuberculosis.
, ventral fluid collection (Arrows). WK = vertebral body. References: Manifestationen der extrapulmonalen Tuberkulose- F Marti, T Bregenzer")
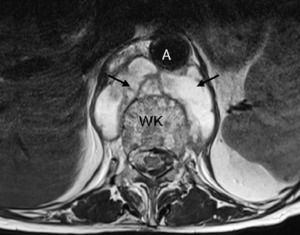
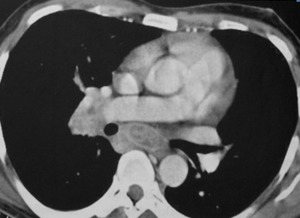
Fig. 21:
Aorta (A), ventral fluid collection (Arrows). WK = vertebral body.

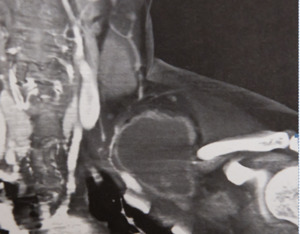
Fig. 22:
Destruction of L1 and basis of Th12.

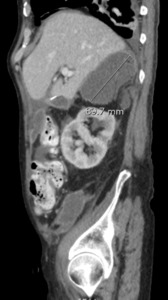
Fig. 23:
Wet type tuberculous peritonitis. Contrast-enhanced CT scan shows ascites.

Fig. 24:
Patient affected by Tuberculosis.

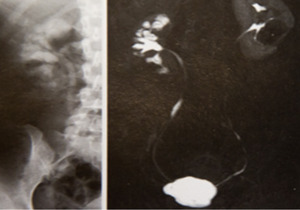
Fig. 25:
Ileocecal tuberculosis. Image from a double-contrast barium enema examination...

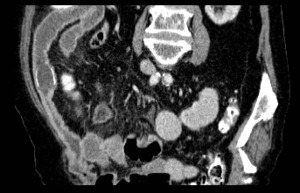
Fig. 26:
Patient affected by Tuberculosis. Contrast-enhanced CT scan shows wall...

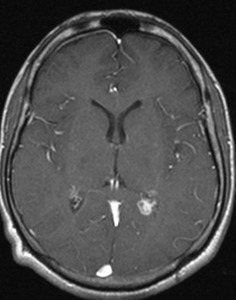
Fig. 27:
MRI 24 year old patient affected by Tuberculosis -T1 SE Transversal.

Fig. 28:
MRI 24 year old patient affected by Tuberculosis -T1 SE Transversal.

Fig. 29:
43 year old patient affected by Aspergillosis after Tuberculosis Infection.

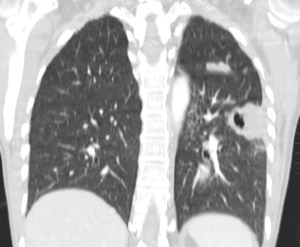
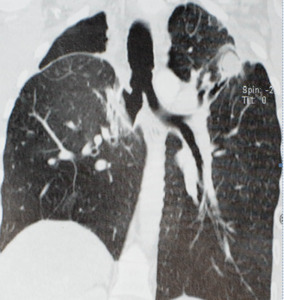
Fig. 30:
55 year old patient presenting Nodules in the Lung after a Tuberculosis...

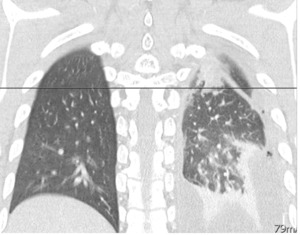
Fig. 31:
48 year old patient presenting lung tumor after Tuberculosis infection.

Fig. 32:
37 year old HIV affected patient with Lymphadenopathy, after diagnostic was...