ECR 2019 / C-2003
Radiomic evaluation of treatment response in patients with glioblastoma: a preliminary study
Congress:
ECR 2019
Poster Number:
C-2003
Type:
Scientific Exhibit
Keywords:
Cancer, Computer Applications-Detection, diagnosis, MR, Neuroradiology brain, CNS, Artificial Intelligence
Authors:
M. D. Patel1, J. Zhan2, K. Natarajan1, R. Flintham3, N. Davies 3, P. Sanghera1, A. Peet1, V. Duddalwar4, V. Sawlani1; 1Birmingham/UK, 2Qingdao/CN, 3Birmingham /UK, 4Los Angeles/US
DOI:
10.26044/ecr2019/C-2003
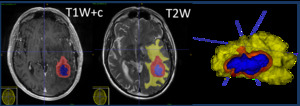
 and peritumoural oedema (yellow). Volumes of interest created (right).")
Fig. 2:
Co-registration of T1-weighted post-contrast and T2-weighted MRI images with...