Anatomy of the nasopharynx
The nasopharynx is the uppermost portion of the pharynx,
extending from the skull base to the soft palate ( Fig. 1 ,
Fig. 2 ).
Its limits are:
- Superior: the sloping base of the skull.
- Inferior: The soft palate,
separating it from oropharynx.
- Posterior: The clivus and the two first cervical vertebrae.
- Anterior: Nasal cavity.
- Lateral: torus tubarius and Rosenmuller recessus
Normal cranial nerves in ceMRN
ceMRN can demonstrate the course,
shape of extracranial branches of the cranial nerves,
which presented high signal intensity with background suppression.
PS: According to the macromolecular characteristics of the contrast agent,
it is blocked by the blood-nerve barrier (BNB) from nerve tissue but remains in a venous plexus to be absorbed by soft tissues,
such as muscle and salivary gland.
Consequently,
the peripheral nerve remains relatively hyperintense on this heavy T2W images due to the binding water in small molecule protein inside the nerve fiber,
whereas the signal intensity of other soft tissues is evidently suppressed as a result of shortening of T2 relaxation time.
The normal characteristics of peripheral nerves in ceMRN are shown in Fig.
3,
Fig. 4 and Fig. 5

Fig. 3: Summary of MRI characteristics of normal peripheral nerves in ceMRN
Demographics of nasopharyngeal carcinoma
Nasopharyngeal carcinoma is common in Southeast Asia,
especially in Southern China,
however,
it is a relatively rare disease in Europe and the United States [1].
The current standard treatment modality for NPC is radiotherapy alone for early stage and combined radiotherapy and chemotherapy for locally advanced diseases.
Patterns of spread and clinical presentation of NPC
Clinical presentations of NPC are correlated with the extent of primary lesion and lymph nodes metastasis.
Most common routes of primary tumor invasion are:
- Anterior: the nasal cavity,
pterygoid fossa,
and maxillary sinuses;
- Lateral: involvement beyond the pharyngobasilar fascia into the parapharyngeal and infratemporal spaces;
- Posterior: base of skull,
clivus and longus scapitis;
- Superior: intracranial structures
Hence,
depending on the anatomical structures affected,
clinical presentation varies accordingly:
- Epistaxis
- Unilateral nasal obstruction
- Auditory complaints
- Cranial nerve palsies (III,
V,
IX,
and XII being most affected).
Nodal metastasis in the neck is a frequent clinical manifestation in NPC,
occurring in roughly three-quarters of all patients[2].
The accurate TNM staging of NPC plays an important role in clinical diagnosis,
treatment planning,
prognosis.
The seventh edition AJCC staging systems is detailed in Fig.
6.

Fig. 6: The seventh edition AJCC staging systems of NPC
References: Pan, J., et al., A Comparison Between the Chinese 2008 and the 7th Edition AJCC Staging Systems for Nasopharyngeal Carcinoma. American Journal of Clinical Oncology, 2015. 38(2): p. 189-196.
Once cranial nerves is involved,
it is classified as T4,
perineural tumor spread(PNS) is an insidious and it may progress upward and backward to the cavernous sinus and middle cranial fossa through nerves foramina.
It invades cranial nerves oculomotor nerve (III),
trigeminal nerve (V),
glossopharyngeal nerve (IX),
and hypoglossal nerve (XII).
Among these,
the maxillary(V2),
mandibular(V3),
IX and XII are the most commonly involved.
Imaging findings on MRI:
- Nerve enhancement
- Nerve enlargement
- Expansion of the neural foramen or canal
- Obliteration of the fat planes
- Erosion or destruction of the skull base foramina
- In ceMRN,
additional information of abnormal cranial nerves are listed in Fig.
7

Fig. 7: Summary of MRI characteristics of abnormal peripheral nerves in ceMRN
Review anatomy of the trigeminal nerve (V) and its branches:
The trigeminal nerve is the largest cranial nerve which leaves the pons in a rather lateral position.
It courses straight through the pre-pontine cistern to enter the Gasserian ganglion.
The skull base segment of the trigeminal nerve then emerges from the Meckel’s cave where the Gasser ganglion is located towards the exit foramina of its three peripheral branches: ophthalmic,
maxillary and mandibular nerves,
and beyond the foramina the peripheral segment can be found.
The three branches course as follow Fig. 8 :
- The ophthalmic nerve (V1) arises from the anteromedial region of the Gasserian ganglion,
passes through the lateral wall of cavernous sinus and divides into three branches (lacrimal,
frontal,
and nasociliary nerves) immediately before entering the superior orbital fissure.
- The maxillary nerve (V2) reaches out from Meckel's cave passing straight through foramen rotundum,
then turns laterally into the upper pterygopalatine fossa (PPF) and inferior orbital fissure before bending anteriorly into the orbit,
through the infraorbital groove,
where it gives rise to the zygomatic and the infraorbital nerves.
Then it reaches to the outside and looking down,
this double angulation has a particular bayonette-shaped axial cutting to get into the infraorbital nerve canal and the zygomatic nerve passes along the lateral orbital wall,
exits the orbit laterally,
and pierces the temporal fascia.
- The mandibular nerve (V3) passes under the Gasser ganglion coming out of the skull through the foramen oval.
Then it gives rise to small motor anterior trunk and another sensory posterior trunk.
The posterior trunk divides into three branches: auriculotemporal,
lingual,
and inferior alveolar nerves.
Review anatomy of the glossopharyngeal nerve (IX):
The glossopharyngeal nerve emerges from the lateral medulla into the lateral cerebellomedullary cistern above the vagus ,
parallel to the vagus nerve and spinal nerve.
Passes through nervous pars of jugular foramen and comes to the nasopharyngeal space.
( Fig. 9 )
CASES
Case 1:
A male,
50-year-old patient presented with masticatory atonia 2 months ago,
then developed numbness of the right mandible and right mouth angle,
and gradual progressed to muscular atrophy of the right temporal and buccal region for 1 month.
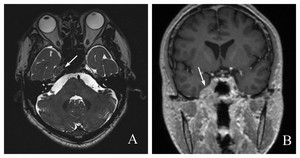
Fig. 11: A: axial T2 space sequence shows a soft tissue lesion in enlarged right Meckel’s cave (arrow), and the hyperintense of cerebrospinal fluid (CSF) disappeared
B: coronal contrast enhanced T1WI shows the lesion along right trigeminal nerve path obviously enhanced (arrow)

Fig. 12: A: oblique coronal ceMRN (MIP thickness=10mm) shows two main branches of right mandibular nerve (V3), the lingual nerve (short arrow) and the inferior alveolar nerve (long arrow), thickened and intensity increased.
B: biopsy of nasopharynx proved it is non-keratinising undifferentiated carcinoma
Case 2:
A 38-year-old female,
present headache for 2 months,
dysphagia for 2 weeks,
when sticking her tongue out,
it points to the right.
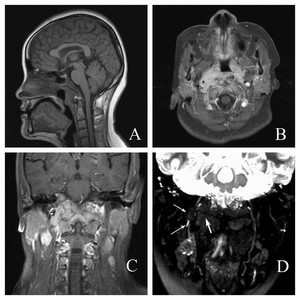
Fig. 13: Sagittal T1WI (A), axial (B) and coronal (C) contrast enhanced T1W fs images present the tumor invade bilateral parapharyngeal space, longus scapitis, pharyngobasilar fascia and clivus
D: coronal ceMRN (MIP thickness=10mm) shows right glossopharyngeal nerve (thin arrow) embodied by enlarged lymph nodes partly, and right hypoglossal nerve (thick arrow) has been embodied by the mass completely
After two months of radiotherapy and chemotherapy,
the volume of primary tumors and enlarged lymph nodes was significantly reduced,
and the patient’s clinical symptom has mainly recovered,
especially masticatory capacity and swallowing function.

Fig. 14: Axial (A) and coronal (B) contrast enhanced T1W fs images shows the residual tumor was significantly reduced
C: coronal ceMRN (MIP thickness=10mm) shows right glossopharyngeal nerve (long arrow) and right hypoglossal nerve (short arrow) become continuous and the signal intensity has been also recovered gradually
Case 3:
A 58-year-old male presented with left nasal obstruction,
left ear hearing loss,
left hard palate numbness and dysphagia for about 2 months.

Fig. 15: Sagittal T2WI (A), axial T1WI (B) and axial T2W SPAIR image (C) present a mass occupied in nasopharynx (the left side of the lesion is more obvious), the posterior nasal obstruction, medial and lateral pterygoid muscle also invaded

Fig. 16: A: oblique sagittal ceMRN (MIP thickness=10mm) shows the left maxillary nerve (V2, arrow shows) thickened, signal intensity increased partly
B: oblique coronal ceMRN (MIP thickness=10mm) shows left mandibular nerve (V3) compressed (short arrow) by the mass, and the proximal part embodied (long arrow) by the mass
C: coronal ceMRN (MIP thickness=10mm) present the left glossopharyngeal nerve (short arrow) and left hypoglossal nerve (long arrow) formed abnormal and embodied by the mass


 and axial (B) T1-weighted images illustrating normal nasopharynx anatomy")
")



