ECR 2019 / C-2018
Ultrasonographic laryngeal anatomy and dynamic evaluation: how to do it
Congress:
ECR 2019
Poster Number:
C-2018
Type:
Educational Exhibit
Keywords:
Motility, Education and training, Education, Ultrasound, MR, Head and neck, Ear / Nose / Throat, Anatomy
Authors:
A. Sorrentino1, F. Rosa1, I. Verardo1, C. Martinetti2, G. Buonomenna1, A. P. Sampieri1, G. peretti1, G. Cittadini2, C. E. Neumaier1; 1Genova/IT, 2Genoa/IT
DOI:
10.26044/ecr2019/C-2018

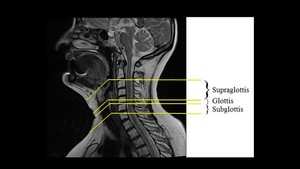
Fig. 1:
Partition of the larynx

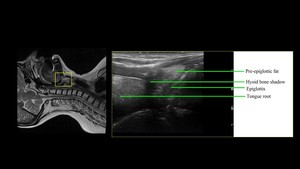
Fig. 2:
Structures of the Supraglottis

Fig. 3:
Structures of the Supraglottis

Fig. 4:
Structures of the Supraglottis

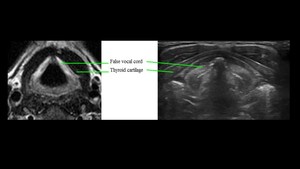
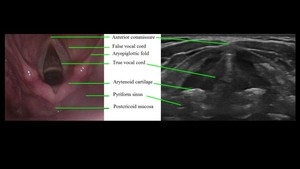
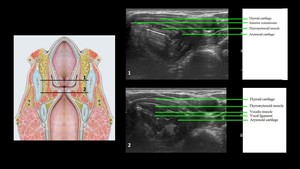
Fig. 5:
Structures of the Supraglottis and Glottis

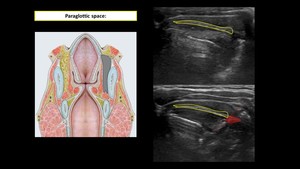
Fig. 6:
Anterior and posterior Paraglottic Space

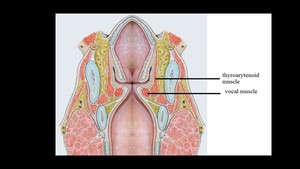
Fig. 7:
Thyroarytenoid and Vocalis muscle

Fig. 8:
Thyroarytenoid and Vocalis muscle

Fig. 9:
The Glottis

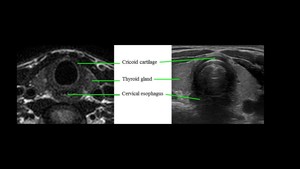
Fig. 10:
The Subglottis

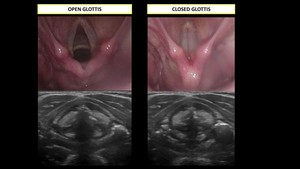
Fig. 11:
Open and closed Glottis