Results
Daniel Kahneman`s consolidated finding is summarized in fig.
1,
every human individual is coming to a decision on two different ways,
either intuitively and heuristically on the basis of recalled patterns or using a systematical approach by analytical tools to link up consolidated knowledge critically.
Clinicians under pressure of time adhere to the first one specifying erroneous orders on the imaging department depending on the training level of the requesting clinician.
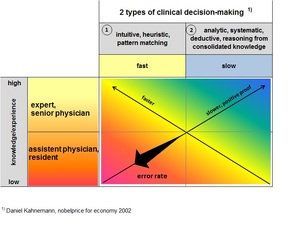
Fig. 1
References: MBM
fig.
1 Clinical decision-making to specify an order on the imaging department
This process forces the imaging department to verify or falsify the requested order ending up all too often to induce multiple radiological exams with the same or a different modality on the same or a different region of organ (sequential diagnostic procedure).
Typical diagnostic sequences with the use of ultrasound (US),
conventional x-ray (CX),
CT und MRI (MR) as practiced by the imaging dept.
of a university clinic,
ist displayed on fig.
2.
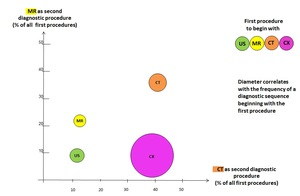
Fig. 2
References: MBM
fig.
2 Repeated use of modalities (diagnostic sequences) in an imaging dept.
of an university clinic
The most frequently used diagnostic sequence starts with CX (diameter),
followed in nearly 40% of all the CX-procedures by CT and in about 10% by MRI.
The second frequent cascade begins with CT followed in about 40% of all of the CT-procedures by CT again and in 35% by MRI.
Even MR-procedures are being followed by CT-procedures in 13% of all of the MR-procedures and by MR-procedures again in 22% of the first MR-procedure.
The trauma surgery and the internal medical disciplines are causing mainly the cascades beginning with CX.
The medical disciplines are principally causing the CT cascades.
There is generally no sense of a CX-sequence with CT as the second procedure as CT is using X-rays to allow for more differentiated diagnosis on the basis of much more information per exam.
The sequential use of CX and CT applies more doses to the patient and extends mostly the duration of treatment.
Most of the sequences are pointing at a deficit of specifying the clinical request for radiological exams to standards as fig.
3 demonstrates benchmarking 2 secondary hospitals,
the left one with a trauma center and the right one centering internal medicine.
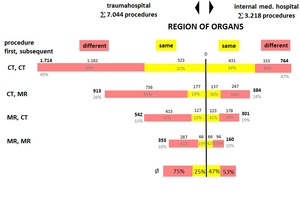
Fig. 3
References: MBM
fig.
3 Diagnostic sequences with CT,
MRT with the same residential treatment
(2 secondary hospitals of the same size)
To read fig 3,
on the same hospital stay a specific organ of a patient is treated by CT and later on (up to 10 days) a different organ again by CT (red color).
This process applies also to the same organ (yellow color).
Fig.
3 reveals these sequential procedures for CT and MR as first and second procedures appropriately.
The last line gives the average result for all of the above procedures.
Typically the trauma oriented procedures work stepwise to begin with the examination of one organ region (25%) followed by different ones (75%).
And this takes time as fig.
4 indicates.
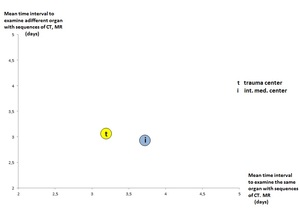
Fig. 4
References: MBM
fig.
4 Average time gap for sequential procedures with CT,
MRT
Fig.
3 and 4 clearly indicate a lack of systematic clinical examination.
The latter would avoid diagnostic sequences particularly on different organ regions with a time lag of days.
This always will extend the duration of hospital stay,
increase the clinical and radiological treatment effort as well as the discomfort for the patient and finally will increase the total cost of residential treatment per patient.
To estimate the cost-effect of unnecessary diagnostic procedures it is to differentiate between the effect on the clinical and the radiological treatment.
The latter relates to cost for staff and consumables,
the first one to the average cost for additional hospitalization.
Restrictions concern trauma and oncology treatment with the necessity of multiple exams of the same organ region before,
during and after treatment.
The analysis of RIS-data from 45 clinics indicates obsolete multiple radiological exams of the same organ region of about 1/3 and of different organ regions of 50%.
The percentage of multiple procedures with CX,
CT,
MRT differs between the analysed hospitals from 30% to 60%.
This analysis is based on 50% and on an average time delay between the sequential procedures of 2,5 days.
The cost for an additional day of stay is estimated to € 250 (about 50% of actual cost as treatment is postponed until identification of patient’s problem),
CMI is assumed to one.
To calculate the appropriate cost savings for the imaging dept.
the cost of staff per procedure is needed as well as the amount of consumables.
These figures are to be multiplied with the obsolete procedures.
The total possible savings are summing up between 30% and 40% of the total cost of the imaging department including cost of depreciation of the respective modalities.
Of these savings the contribution of additional hospitalization varies between 60% und 75%,
i.
e.
the savings of the imaging dept.
contribute to the total cost savings between 40% and 25% respectively.


