Definition: AML is a solid benign tumor composed of varying proportions of adipose tissue,
smooth muscle and abnormal blood vessels.
Epidemiology: AMLs are more frequent in woman than in man(4:1) with a peak of incidence between the fourth-sixth decades of life[1].
Clinic: Most commonly AMLs are asymptomatic,
but lesions>4cm can present with retroperitoneal hemorrhage due to tumor rupture and severe symptoms as:
- anemia
- hematuria
- flank pain
- palpable mass
- renal failure
Histology: Although once considered a hamartoma,
AML is now considered among the family of perivascular epithelioid cell tumors(PEComa)[2] and classified histologically as:
1.
typical(triphasic) AML-well circumscribed and encapsulated
masses with variable amount of fat,
numerous blood vessels
without internal elastic membrane and disorganized smooth muscle
pattern;
- subtype with low fat content,
defined as fat content less than 25%/fhp
- subtype entity with epithelial cysts.
2.
atypical(epithelioid) AML-masses composed of numerous ephiteloid
muscle cells with nuclear pleomorphism,
low fat but no blood
vessels.
Imaging methods
1.Ultrasound(US)–used as primary imaging tool.
It is safe,
reproducible
and inexpensive but it dependent on operator/body habitus of the patient.
2.Computed tomography(CT)–the most commonly imaging method
having higher precision/reproducibility,
minimizing inter- and intraobserver variability and preferable for pre-surgical mapping prior to embolization.
Its use in the diagnosis/follow-up of patients is limited by the accumulation of radiation.
3.Magnetic resonance imaging(MRI)-is sufficient to assess the size of AML/other renal lesions even without contrast.
Does not radiate and thus enables good characterization of lesions.
Its spatial resolution is lower than that of CT,
because of the artefacts caused by abdominal movements that blur lesions and organ contours.
Typically AMLs contain sufficient amounts of macroscopic fat that can be accurately diagnosed using CT/MRI.
In some cases,
they may contain microscopic fat,
hardly to detect on imaging,
known as fat-poor type.
The radiological classification of AMLs based on specific imaging features,
histologic and clinical includes firstly two major categories: sporadic(Table 1) and hereditary(TSC)[3].
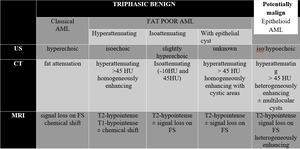
Table 1: Imaging features of renal AML, adapted after Jinzaki M, Silverman SG, Akita H, et al.
A recent article[4] proposed a classification of AML using CT and MRI findings using quantitive values (ROI,
TSR and SII),
as fat-rich,
fat-poor and fat-invisible(Table 2).
Table 2. Radiological classification of AML,
adapted after Song S
| |
NECT
region of interest |
MRI-CSI tumor-to-spleen
ratio(TSR) |
MRI-CSI signal
intensity index |
| fat-rich AML |
<-10 HU |
<0.71 |
>16.5% |
| fat-poor AML |
>-10 HU |
<0.71 |
>16.5% |
| fat-invisible AML |
>-10 HU |
>0.71 |
<16.5% |

