Trauma
Hematoma and Vascular Injuries
Hematomas can develop from blunt or penetrating trauma or complicate surgery or other invasive procedures.
Vascular injuries range from intimal tears to transections or occlusions.
Displaced fracture fragments into the axilla or axillary hematoma should prompt careful examination of the axillary blood vessels.
Key imaging findings:
- Collection with poorly-defined margins (hematoma)
- Usually high attenuation when acute but become more heterogeneous over time
- Filling defect,
occlusion,
or pseudoaneurysm (vascular injury)
- Displaced fracture fragments from ribs,
scapula,
humerus,
or clavicle
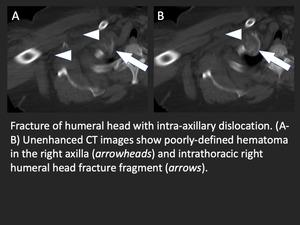
Fig. 2: Axillary hematoma from humeral head fracture dislocation
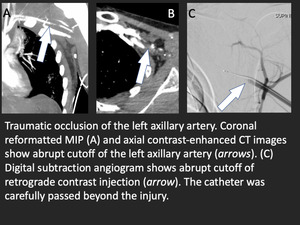
Fig. 3: Traumatic axillary artery injury
Seroma and lymphocele
Seromas and lymphoceles can develop following axillary surgery,
especially surgeries for breast cancer.
Most require no management,
and CT is usually diagnostic. Ultrasound or MRI can be used for unclear cases.
Key imaging findings:
- Well circumscribed axillary collection
- Homogeneous water attenuation
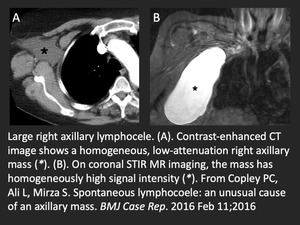
Fig. 4: Spontaneous axillary lymphangioma.
References: Copley PC, Ali L, Mirza S. Spontaneous lymphocoele: an unusual cause of an axillary mass. BMJ Case Rep. 2016 Feb 11;2016
Vascular
Hemangioma
Hemangioma is a benign vascular mass containing smooth muscle cells,
fat,
and fibrous tissue.
They are usually identified incidentally in the axilla but can present as a palpable mass.
Key imaging findings:
- Heterogeneous tissue mass with small calcifications (phleboliths)
- Mixed types may have anomalous draining veins
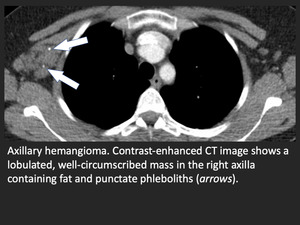
Fig. 5: Axillary hemangioma
Vascular occlusions and stenoses
Occlusion or stenoses of the axillary artery or axillary vein can result from coagulopathy,
trauma, instrumentation,
or thoracic outlet syndrome.
Upper extremity venous thrombosis can propagate into the axillary vein,
and thrombi from the heart and proximal aorta can embolize into the axillary artery.
Key imaging findings:
- Vascular filling defect(s) or occlusion
- Edema in the adjacent fat (suggesting thrombophlebitis)
- Collateral vessels indicating chronicity (especially in patients with dialysis arteriovenous fistulae)
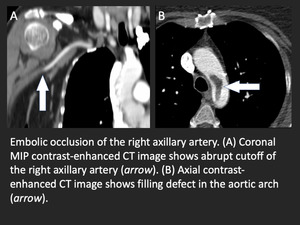
Fig. 6: Embolic axillary artery occlusion
Lymphadenopathy
Lymphadenopathy is one of the most common abnormalities found in the axilla on chest CT.
It can be reactive,
infectious,
or malignant.
Occasionally,
normal venous valves can be mistaken for lymphadenopathy,
especially when the axillary vein is distended.
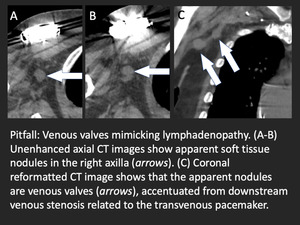
Fig. 7: Pitfall: venous valves mimicking lymphadenopathy
Reactive
Silicone particles from breast implants or free injection can cause a granulomatous reaction within lymph nodes.
Similarly,
reactive high attenuation lymph nodes can develop in patients with extensive upper extremity and upper torso tattoos as a result of gradual accumulation of ink particles in the lymphatics. While lymphadenopathy is one of the hallmarks of sarcoidosis,
axillary involvement is uncommon.
Key imaging findings
- High attenuation lymph nodes (silicone or tattoo ink)
- Symmetric axillary,
mediastinal,
and hilar lymphadenopathy and perilymphatic lung nodules (sarcoidosis)
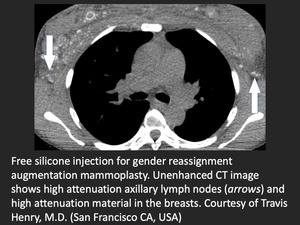
Fig. 8: High attenuation lymph nodes from accumulation of free silicone
References: Travis Henry, M.D., University of California San Francisco (San Francisco, USA)
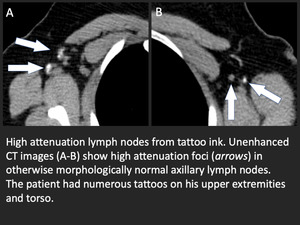
Fig. 9: High attenuation lymph nodes in patient with many upper extremity and torso tattoos.
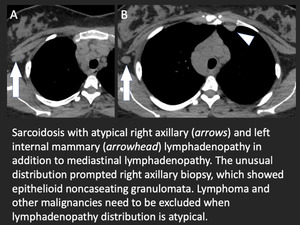
Fig. 10: Atypical distribution of lymphadenopathy in sarcoidosis.
Infection
Common infectious causes of axillary lymphadenopathy include tuberculosis,
cat scratch disease (Bartonella henselae),
sporotrichosis (Sporothrix schenckii),
and infectious mononucleosis (Epstein-Barr virus).
TB lymphadenitis should be strongly considered in patients with necrotizing lymphadenitis who are from or have visited TB-endemic countries.
Key imaging findings
- Central low attenuation suggesting necrosis
- Edema in the adjacent fat
- Bilateral involvement suggests viral infection (mononucleosis)
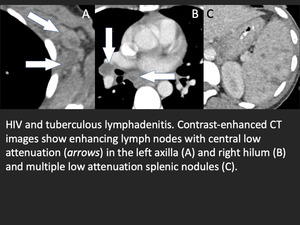
Fig. 11: TB lymphadenitis
Lymphoproliferative disorders
Lymphoproliferative disorders are a common cause of unilateral or bilateral axillary lymphadenopathy and range from reactive polyclonal lymphocyte proliferation to high-grade lymphoma.
Key imaging findings
- Diffuse thoracic lymphadenopathy favors chronic lymphocytic leukemia
- Unilateral lymphadenopathy favors lymphoma
- Hypervascular lymphadenopathy (hyaline vascular Castleman disease or angiofollicular lymphoid hyperplasia)
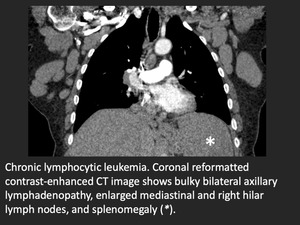
Fig. 12: Chronic lymphocytic leukemia with bilateral axillary lymphadenopathy
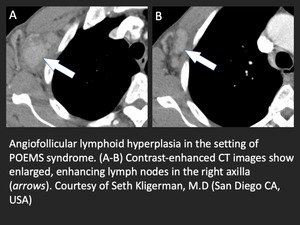
Fig. 13: Angiofollicular lymphoid hyperplasia in the setting of POEMS syndrome
References: Seth Kligerman, MD, University of California San Diego, San Diego, USA
Metastases
The axilla is also a common site for metastasis,
especially from breast malignancies and melanoma.
Key imaging findings
- Lymph node enlargement with loss of normal fatty hilum
- Varying degrees of contrast enhancement or low attenuation
- Coalescence of affected lymph nodes
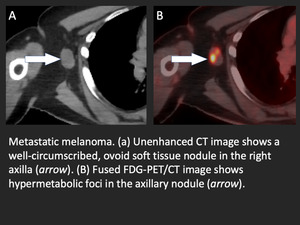
Fig. 14: Axillary lymph node metastasis from melanoma
Musculoskeletal
A palpable axillary mass is a common indication for chest CT. A variety of soft tissue masses can develop in the axilla,
ranging from benign lipoma to an aggressive sarcoma.
Lipoma and liposarcoma
Lipoma is a benign,
well-circumscribed homogenous mass formed from adipose tissue.
Liposarcoma is a malignant mass of neoplasitc adipose cells and varies in degree of differentiation and grade.
Key imaging findings:
- Lipoma - well circumscibed mass,
nonenhancing mass of pure fat attenuation
- Liposarcoma - infiltrating,
heterogeneous mass with varying degrees of adipose tissue and contrast enhancement
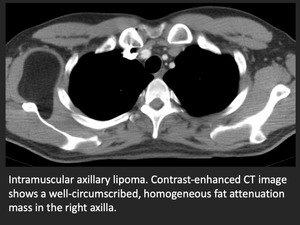
Fig. 15: Axillary lipoma
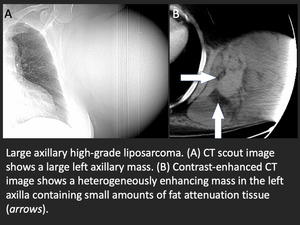
Fig. 16: Axillary liposarcoma
Hibernoma
Hibernoma is a rare benign mass that consists of brown fat.
Hibernomas can mimick liposarcoma on imaging.
In contrast to liposarcomas,
hibernomas have characeristic small,
spertine blood vessels coursing through the mass.
Key imaging findings:
- Heterogenous mass with serpentine internal vasculature
- FDG avid on PET/CT
Desmoid (fibromatosis)
Desmoid tumor is a benign but invasive mass of fibrous tissue and has a high rate of recurrence after resection.
Desmoids can invade the blood vessels and nerves in the axilla owing to their infiltrating nature,
making resection very difficult.
Key imaging findings:
- Infiltrating homogeneous mass
- Attenuation similar to that of skeletal muscle
- Enhances following contrast administration
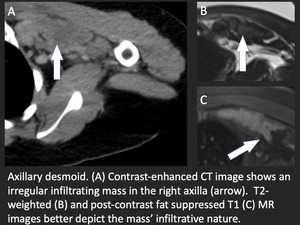
Fig. 18: Axillary desmoid
Neurologic
Axillary pathologies of neural origins are rare.
Brachial plexopathy can result from trauma or peripheral nerve sheath tumors such as schwannoma or neurofibroma,
metastases,
aneurysms,
infection,
or thoracic outlet syndrome.
Axillary neurofibromas can occur in isolation or more commonly develop in the setting of neurofibromatosis (NF).
Plexiform neurofibromas can present as large axillary masses following the neurovascular bundles.
Key imaging findings:
- Homogeneous infiltrating axillary mass
- High T2-signal intensity and contrast-enhancement on MRI
- Other masses (paraspinal,
intercostal) should suggest NF-1
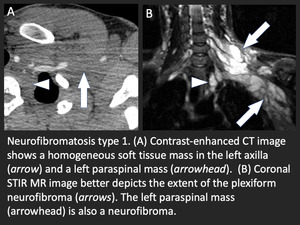
Fig. 19: Axillary plexiform neurofibroma in the setting of neurofibromatosis type 1.
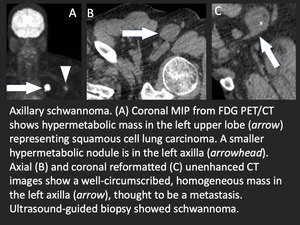
Fig. 20: Axillary schwannoma initially thought to be lymph node metastasis in patient with squamous cell carcinoma of the lung
Breast tissue
The prevalence of accessory breast tissue ranges from 0.6%-6.0% and is most commonly found in the axilla.
Patients may present with a palpable mass that exhibits cyclic hormonal changes.
Fibroadenoma and hamartoma are benign breast masses that rarely occur in accessory breast tissue.
Furthermore,
primary breast cancer,
oil cysts,
and fat necrosis may also develop in the accessory axillary breast tissue.
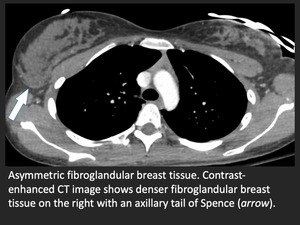
Fig. 21: Asymmetric breast tissue with axillary tail of Spence.
Skin
A few common benign skin lesions can be seen in the axilla including sebacceous cysts and epidermal inclusion cysts.
Axillary cellulitis can cause skin thickening on CT,
and the underlying axillary fat may be edematous.
Hidradenitis suppurativa
Hidradenitis suppurative is a rare, chronic skin disorder characterized by subcutaneous abscesses,
sinus tracts,
and scar tissue. The axilla, groin,
buttocks,
and inframammary regions are most commonly affected. Females are affected more commonly than males.
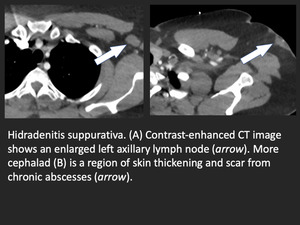
Fig. 22: Axillary hidadrenitis suppurativa

. The axillary space includes the axillary sheath and lymph nodes. Lymph nodes are classified with respect to pectoralis minor. Nodes lateral to the muscle are level I, nodes underlying the muscle are level II, and nodes medial to the muscle are level III.")