Introduction
Extra-testicular lesions may present as scrotal masses or incidental findings. They can originate from epipidymis,
spermatic cord or tunica vaginalis,
with each of these structures potentially affected by a variety of pathologic processes.
Ultrasonography (US) with a high-frequency transducer (8-15 MHz) is the first choice of diagnostic imaging of scrotal masses.
US is able to identify and characterise intratesticular or extratesticular lesions,
may distinguish between benign or malignant lesions and identify conditions requiring emergent surgical intervention.
Majority (97%) of extra-testicular lesions (as opposed to intra-testicular masses) are benign.
Most extra-testicular lesions originate from or are dependent on the tunica vaginalis.
Anatomy
Deep to the scrotal skin lies the fibromuscular scrotal sac,
divided into the right and left hemiscrotum by a midline septum (raphe).
Each sac contains a testis,
epididymis,
spermatic cord and associated fascial coverings.
The male testicle is an ovoid structure measuring with a homogeneous echogenicity (Fig. 1). The epididymis is a comma-shaped,
isoechoic tubular structure along the posterior testicle border.
The epididymal head overhangs the superior pole of the testicle with the body and tail behind and along the inferior pole of the testicle.
The tail of the epididymis continues as the vas deferens in the spermatic cord.
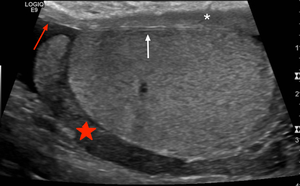
Fig. 1: Normal Testes and epipidymal body.
Testicle is covered by the tunica vaginalis (white arrow). The inner aspect of the scrotal wall (asterisk) is covered by the tunica albuginea (red arrow). The epididymal body (red star) is coarser in echotexture compared to the testes.
Testes and epididymides are protected from external injury by the fibrous covering,
the tunica albuginea,
seen as a thin echogenic band.
The tunica albuginea is covered by the tunica vaginalis,
a remnant of the processus vaginalis,
consisting of two layers.
The visceral layer lines the tunica albuginea and is separated by the parietal layer lining the inner scrotal wall by an interspace containing small amount of fluid.
The vas deferens courses cranially within the inguinal canal as part of the spermatic cord.
In addition to the vas deferens,
the spermatic cord contains; nerves,
lymphatic ducts,
arteries and the pampiniform venous plexus.
On US the spermatic cord appears as a highly echogenic band within the inguinal canal.
Scrotal Embrology
The development of viable spermatozoa require the testes to descend into the cooler environment of the scrotum.
Testes descend from their intra-abdominal location through the anterior abdominal wall into the scrotum along the inguinal canal pathways facilitated by the gubernaculum ligament (Fig. 2).
The processus vaginalis is a sac-like evagination of the abdominal wall providing an communication between the peritoneum and scrotal folds following the regressing gubernaculum.
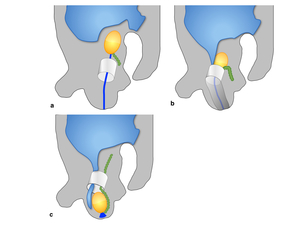
Fig. 2:
Diagrammatic depiction of embryologic development of the inguinal canal.
a. Age: 7/40 weeks gestation. The gubernaculum passes through the anterior abdominal wall into the developing inguinal canal. Gubernaculum is attached to the inferior pole of the extra-peritoneal testes and distally to the labroscrotal folds.
b. Age: 26-28 /40 weeks gestation. The gubernaculum shortens, facilitating the testis descent through the deep inguinal ring. Testicular descent takes 2 - 3 days to pass through the inguinal canal. Processus vaginalis extends through the anterior abdominal wall along the path formed by the gubernaculum. The invagination extends the abdominal wall layers that in turn from the scrotal walls and the spermatic cord.
c. Age: 32 -40 / 40 weeks gestation, the inguinal canal forms, with a gradual obliteration of the processus vaginalis .
The evagination extends the abdominal wall layers,
these layers will in turn form the inguinal canal walls and ultimately contribute to the final the scrotal layers and the spermatic cord (Fig. 3).
The opening of the transversalis fascia becomes the deep inguinal ring.
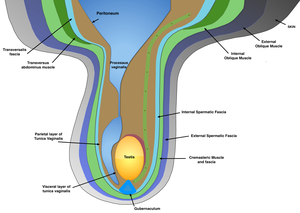
Fig. 3: The first layer to evaginate is the transversalis fascia, lying deep to the transverse abdominus muscle. This layer becomes the internal spermatic fascia, the inner most layer of the sheath; the internal oblique muscle forms the cremaster muscle, the intermediate layer; and the external oblique muscle gives rise to the external spermatic fascia, the outermost layer (5). These fascial layers are invested within a fibromuscular sac that contains the dartos muscle.
Hormonal changes obliterate the proximal processus vaginalis once testicular migration is completed.
The remaining processus vaginalis covers the testes forming the tunica vaginalis.
Most extra-testicular lesions originate from or are dependent on the tunica vaginalis (6).
This fascial structure normally covers the entire testis bar the posterior border with a visceral layer covering the testes and a peripheral parietal layer lining the internal spermatic fascia of the scrotal wall.
Ultrasound Technique
Thick gel application creates a stand-off to reduce compression zone artefacts (including hair artefacts) and optimises superficial lesions.
Scanning is performed with a high-frequency 8 - 15 MHz transducer with virtual convex setting at 2-3 focal zones.
Higher frequency probes allow for greater resolution of the scrotal contents,
whilst lower frequency probes can be used to penetrate through oedematous scrotums and deep hydrocoeles.
Sequential longitudinal and transverse images are acquired.
Dual images allow comparison of echo texture and vascularity of left/right.
Developmental extra-testicular anomalies:
The obliteration of the processus vaginalis is important,
as when incomplete,
it results in different types of congenital abnormalities.
A patent processus vaginalis is the cause of both a congenital spermatic cord hydrocele or an indirect inguinoscrotal hernia.
Spermatic cord hydrocele
Definition: Aberrant closure of the processus vaginalis results in lobulated fluid collection along the spermatic cord.
Clinical Presentation: Groin swelling that is indistinguishable from a mass.
- Key US findings: Oval anechoic mass in the groin along the spermatic cord,
positioned above and separated from the testis and epididymis.
Well-demarcated.
- Avascular on doppler interrogation.
Three subtypes
Communicating hydrocele
Complete patency of the processus vaginalis.
- Key US findings: fluid collection extends from the pelvis through the deep inguinal ring to the scrotum.
Similar US appearance to an acquired hydrocele.
Funicular hydrocele
Abnormal obliteration of the deep inguinal ring,
with the normal constriction just above the testis ( Fig. 4 ).
- Key US findings:: Fluid collection communicates with the peritoneum at the internal inguinal ring,
but does not communicate with the tunica vaginalis.
Remnants of partial constrictions can result in a beaded appearance.
- Size increases with a corresponding increase in intra-abdominal pressure.
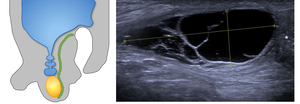
Fig. 4: Funicular hydrocele
5yr presented with 2 weeks of swelling within the spermatic cord.
Diagrammatic representation of a funicular hydrocele US grey scale demonstrates oval anechoic mass along the spermatic cord. Positioned above the right testes and epididymis (asterisk). Avascular on doppler Fluid collection communicates with the peritoneum at the internal inguinal ring, but not with the tunica vaginalis If it does not spontaneously regress, elective surgery is useful to prevent an acquired indirect hernia.
Encysted hydrocele
Fluid collection is enclosed between the constrictions at the deep inguinal ring and just above the testes.
It does not communicate with the peritoneum or tunica vaginalis ( Fig. 5 ).
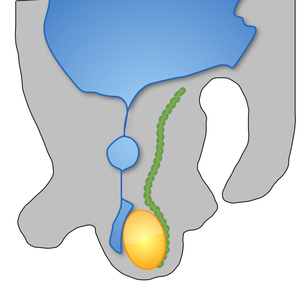
Fig. 5: Diagrammatic representation of an encysted hydrocele. Both the testis and epididymis will remain separate from the fluid.
Indirect Inguinoscrotal hernia
Definition: Intestinal loop or omentum passes into the scrotal cavity through an incompletely obliterated processus vaginalis at the deep ring.
Hernia courses anteromedially to the spermatic cord and emerges through of the superficial ring,
descending into the scrotum ( Fig. 6 ).
Clinical Presentation: Groin bulge often associated with pain/dragging sensation,
exacerbated by increasing intra-abdominal pressure. Often resolves when the patient is supine.
- Key US findings: Tubular structures containing moving gas representing peristalising bowel loops.
Omentum appears as an elongated,
highly echogenic structure with branching vessels on colour dopper.
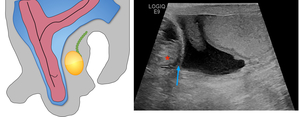
Fig. 6: 30 year old male presented with a right inguinal swelling. Clinical exam demonstrated it was irreducible hernia. Diagrammatic representation of an inguinoscrotal hernia Ultrasound to assess for hernial contents. US grey-scale demonstrates herniation of peritoneal fat and peristalising bowel (asterisk) reaching up to the right scrotum (blue arrow)
Varicocele
Abnormal dilatation of pampiniform venous plexus surrounding the spermatic cord.
Primary varicoceles are due to venous reflux into the pampiniform plexus from the internal spermatic vein due to incompetent or congenitally absent venous valves (85% of cases).
The left sided predominance is attributed to the left internal spermatic vein draining into the ipsilateral renal vein at a 90 degree angle,
allows transmission of the renal vein pressure,
which can oppose flow from the internal spermatic vein.
( Fig. 7 )
Clinical Presentation: Scrotal thickening above the testis or symptoms of a dull pain in the scrotum or groin exacerbated by standing or during an erection.
- Key US findings:: Multiple,
tortous,
tubular,
anechoic structures separate to the testis.
- Calibre increases by 2 - 3 mm during Valsalva manoeuvre.

Fig. 7: 35 yr old male with left vague scrotal discomfort.
Schematic figure of a varicoele:
Image a: US grey-scale demonstrates dilatation of the veins of the pampiniform plexus of the right testis.
Image b: Spectral doppler with valsalva manoeuvre demonstrated reflux > 1 second in duration and a further venous dilatation.
Appendages
Epididymal and testicular appendages represent embryologic remnants that can be identified at US,
especially with a hydrocoele.
Usually clinically insignificant unless they tort and cause intense pain.
Five known appendages,
with the three demonstrated in Fig. 8 most likely to undergo torsion.
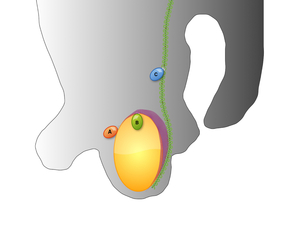
Fig. 8: Schematic diagram of three most common appendages to undergo torsion ;
A: Testicular Appendix, B: Epididymal Appendix, C: paradidymis (Giraldes organ) located on the distal portion of the spermatic cord.
Appendix testis
Vestigial remnant of the Mullerin duct,
known as Hydatid of Morgangi,
located near the head of the epididymis and attached to the tunica vaginalis. 90% of twisted testicular appendices involve the appendix testes.
Key US findings: Often-pedunculate structure from the epididymal head,
isoechoic to testicular tissue.
Fig. 9
Appendix Torsion
Clinical presentation: 10 - 12 year olds with acute scrotal pain.
20% of patients have a classic ‘blue dot’ sign from hemorrhagic infarction Fig. 9.
- Key US findings: Avascular extra-testicular mass with mixed echo texture.
This is often associated with scrotal swelling,
an enlarged epididymal head and a reactive hydrocele.
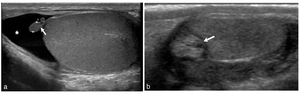
Fig. 9: Image a: Incidental finding in a 24 year old male. US grey-scale image shows a small (5mm) soft tissue remnant projecting from the superior aspect of the testes (white arrow) with a small hydrocele (asterisk).
Image b: 12 year old presented with acute right scrotal pain. US grey scale shows an avascular extra-testicular mass with mixed echo texture (white arrow). No enhanced doppler flow.
The patient underwent surgery which confirmed a torted appendix testis
Appendix epididymis
The appendix epididymis is an embryological remnant of mesonephric ducts at the superior end of the epipidymis.
- Key US findings: Oval structure between the epididymis and testis.
Acquired extra-testicular abnormalities
Acquired Hydrocoele
Abnormal accumulation of serous fluid between the layers of the tunica vaginalis surrounding a testis,
is the most common form of scrotal enlargement Fig. 10.
They are considered either primary or secondary.
Primary hydrocoele is idiopathic either from excessive fluid production or defective fluid absorption.
Secondary hydroceles,
are often associated with an intrascrotal pathology.
Most frequently epididymo-orchitis due to the close proximity of the visercal layer to the testis.
Clinical Presentation: Painless progressing soft fluid-filled,
scrotal mass.
Typically present with impalpable testis,
Acquired hydroceles are often comparably less tense.
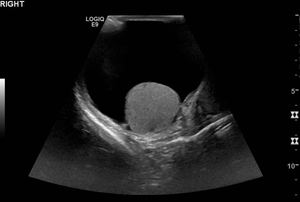
Fig. 10: 56 year old male presents with a painless progressive right scrotal mass.
Key US findings: Simple anechoic fluid collection to a depth of 5cm intimately surrounds the right testis with good sound transmission. The collection is avascular on doppler scanning, no sepations, calcifications or cholesterol. Right testis has a homogenous echotexture with normal doppler flow.
Scrotal Haematocoele
Accumulation of blood within the tunica vaginalis,
most commonly due to blunt injury or iatrogenic complication (inguinal herniorrhaphy).
Key US findings: vary with age,
Fig. 11 .
- Acute :Initially it is slightly echogenic.
- As the hematocle ages appearances become more complex and hypo echoic with septa,
fluid-filled levels and echogenic debris indicating clots.
- Chronic: Heterogenous encapsulated lesion that may calcify and exert mass effect on the testis.
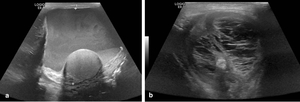
Fig. 11: 66 year presented with scrotal swelling, discomfort and discolouration one day post right inguinal hernia repair. Initial US (image a) demonstrates 7.5 x 6.5cm echogenic fluid collection with dependant layering in keeping with recent haemorrhage. Image b: 32 days post-operative repeat US depicts a complex loculated extratesticular fluid collection with low echogenicity, septa and a fluid-debris level, in keeping with a chronic haematoma. Testicular vascularity was not compromised.
Pyocele
Typically a complication of epididymo-orchitis or testicular abscess.
Clinical Presentation: Scrotal pain and swelling.
Key US findings,
Fig. 12 :
- Complex,
heterogenous fluid collection in the scrotal sac with septa.
Gas,
if present,
may cause hyper echoic foci and shadowing.
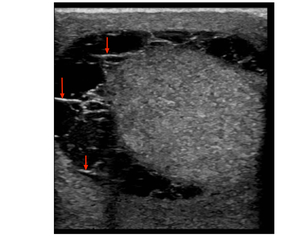
Fig. 12: 18 year old male presented with painful left scrotal swelling. No history of trauma.
US demonstrated enlarged left testis with hypervascularity (doppler image not uploaded). Extra-testicular slender floating echoes and thin internal septa (red arrows) favour pyocele. Patient was referred to urology, the final diagnosis of acute orchitis and an associated pyocele.
Epididymal Cyst
Most common epididymal mass in 20 - 40% of asymptomatic patients. Lymphatic origin,
cysts may contain clear serous fluid,
lymphocytes,
spermatozoa and debris
Clinical Presentation: Often an incidental finding.
Larger cysts present as a palpable mass.
Solitary or approximately 30% multiple
Key US findings,
Fig. 13 :
- Anywhere within the epididymis and appear as well circumscribed anechoic cysts with no internal echoes and posterior acoustic enhancement.
- Larger cysts may contain septations and displace the testis (differentiates cyst from hydrocoele).
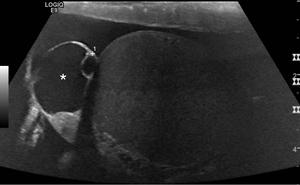
Fig. 13: 45 year old patientspresented with a palpable painless mass scrotal mass.
Image A: 2cm well-defined anechoic epididymal cyst (asterisk) with posterior acoustic enhancement.
Cystic Spermatocele
A cystic dilatation of the efferent ductules tubules in the epididymal head.
thought to be retention cysts or block of the epididymal ducts with an increased incidence after vasectomy.
Clinical Presentation: Usually painless,
incidental finding but can present as a mass lesion if large.
Key US findings Fig. 14 :
- Well-defined epidermal hypo echoic lesions measuring 1 - 2 cm and demonstrating posterior acoustic enhancement.
- Usually irregular,
with fine low-level internal echoes and sometime septations. Can be indistinguishable from epididymal cysts,
often larger.
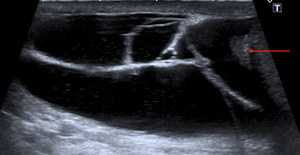
Fig. 14: 56 yr male presented with a palpable painless scrotal mass.
Well-defined hypo echoic lesions and fine internal echoes, separate from the testicle and epididymis (red arrow) .
Spermatoceles are usually larger, irregular shaped cysts containing fine low-level internal echoes and occasionally separations as compared to epididymal cysts.
Epidermoid cyst
Rare (1%),
but benign and well-circumscribed tumours of germ cell origin (1).
Clinical Presentation: Painless scrotal nodule.
Key US findings Fig. 15 :
- Hypoechoic mass with a well defined margin and a central focus of calcification giving a bullseye or target appearance.
- No vascularity demonstrated on colour Doppler imaging.
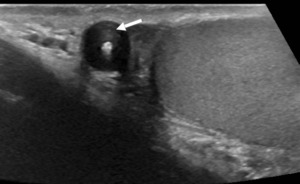
Fig. 15: Epidermoid cyst.
Grey scale image of the left hemi-scrotum.
Well-defined mass with a whorled appearance and a central focus of calcification giving a 'bulls-eye' appearance (white arrow).
No vascularity demonstrated on colour Doppler
Scrotal calculi
Benign incidental extra-testicular macro-calcifications between the layers of the tunica vaginalis Fig. 16.
Thought to result from micro-trauma (particularly to an appendix) or inflammatory diseases affecting the tunica vaginalis.
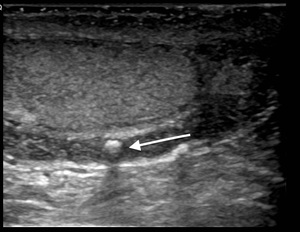
Fig. 16: Scrotal calculi
Incidental finding on testicular US. No recollection of trauma. Mobile hyper echoic calcified body between the layers of the tunica vaginalis (white arrow).
Appearances are typical of a scrotal calculi
Lipoma
Most common para-testicular neoplasm (75%),
most often arising from the spermatic cord. Clinical Presentation: Typically non-tender mass,
can be incidental.
Key US findings Fig. 17 :
- Well-defined,
avascular mass.
- There is variable echogenicity dependent on internal complexity,
this ranges from hyper echoic through to uniformly hypo echoic.
Adenomatoid tumours
Second most common benign tumour of the epididymis,
accounting for 30% of all extra-testicular masses Fig. 18 .
Clinical Presentation: Painless scrotal mass.
Key US findings:
- Typically a smooth,
rounded and well-circumscribed hypo echoic mass.
However as appearances can vary,
the tumour is often resected .
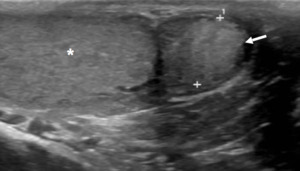
Fig. 18: Adenomatoid
Solid, small (<2 cm) smooth paratesticular ovid lesion with mild hyper-echogencity (arrrow) compared to the epididymal head. Normal testis (asterisk).
No significant colour Doppler vascularity
Absence of serum tumour markers.
Fibrous pseudo tumours
Benign fibroinflammatory reaction involving the tunica albuginea or vaginalis.
Clinical Presentation: Palpable,
painless,
firm and nodular scrotal masses,
which maybe mobile.
Key US findings Fig. 19 :
- Close association to the tunica.
- Variable appearances as a hypo echoic mass with +/- internal calcifications.
- Posterior shadowing suggests dense fibrotic content.
- 50% have an associated hydrocele.
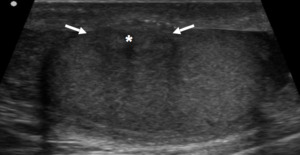
Fig. 19: Fibrous Pseudo tumour
Hypo echoic mass with internal calcifications (asterisk) in close association with the tunica vaginalis (arrows). Posterior shadowing suggests dense fibrotic content. Diffuse plaque like thickening of capsule.
Necrotising Granuloma
Granulomatous disease can manifest as hypo echoic masses with internal vascularity.
Clinical presentation: Rare,
late complication of intravesical BCG treatment.
Often in the context of granulomatous infections such as sarcoidosis.
Key US findings Fig. 20 :
- Heterogeneously enlarged epididymis with hypo echoic area and low blood flow.
- May also have calcifications and a draining sinus.
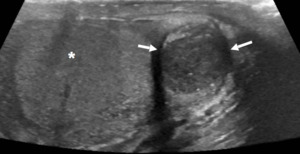
Fig. 20: Necrotising Granuloma
In a patient post-intravesical BCG treatment.
Grey scale US image: Hypo echoic area containing punctate calcifications within an enlarged epididymal head. Doppler demonstrated low blood flow.
Key Benign Imaging Findings
Please see diagram Fig. 21
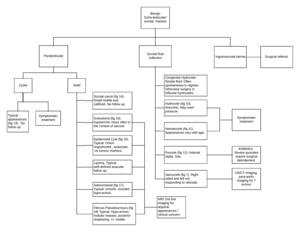
Fig. 21: Flow diagram demonstrating the key US imaging features and treatment of the presented extra-testicular benign masses
Scrotal liposacroma and leiomyosarcoma
These cases are used to highlight some key US differences between malignant and benign lesions .
Scrotal liposarcoma is a rare malignant tumour of male genitalia,
and is often mistakenly diagnosed as an inguinal hernia,
hydrocele and lipoma.
US can be useful to differentiate if from testicular tumour.
Malignant Case One:
Confirmed Liposarcoma Fig. 22
Key US findings:
- Well-defined elliptical lesion in the subcutaneous plane,
abutting the muscle
- Central hyper-echogencity with a peripheral hypoechoic rim.
- No calcification or cysts.
The central echogenicity is due to fat (sutble linear strands).
Worrying feature is the peripheral hypoechogencity.
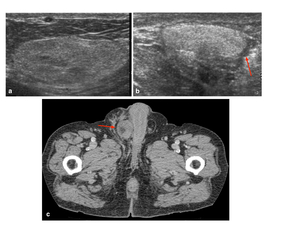
Fig. 22: Histologically proven Liposarcoma.
a: Elliptical well-defined lesion in the right inguinal canal with subtle central hyperechogenic strands.
b: Centrally lesion is hyperechoic and peripherally hypoechoic.
c: CT axial further confirming location and extent of disease.
References: Department of Radiology, University of Trieste, case courtesy of Prof Michele Bertolotto
Malignant Case Two:
Liposarcoma
Key US findings:
- Lobulated hypoechoic lesion within the subcutaneous plane.
- Internal hyperechoic strands.
- Internal flow signals.
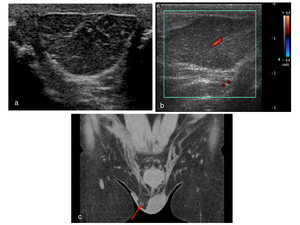
Fig. 23: a: Ovoid heterogenous extratesticular lesion expanding the right spermatic cord and extending down into the scrotum.
b Internal colour doppler flow. The left testis is normal in appearance.
c: Coronal CT confirms soft tissue mass in the right hemiscrotum inseparable from the spermatic cord and allows assessment of associated lymphadenopathy and metastatic deposits.
Histologically proven to represent a liposarcoma of the spermatic cord
References: Department of Radiology, University of Trieste, case courtesy of Prof Michele Bertolotto
Worrying features are the irregular echogenicity and flow signal.
Malignant Case Three:
Leiomyosarcoma Fig. 24
Key US findings:
- Well-demarcated,
predominately hypo-echoic,
heterogenous ovoid lesion remains separate to the testis.
- Avid vascularity on doppler.
MRI findings as depicted and described in the annotation.
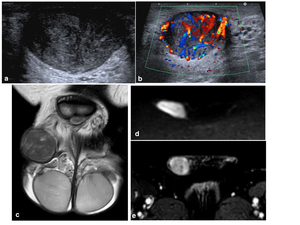
Fig. 24: Histologically proven leiomyosarcoma.
Typically present as a firm, non-tender, rubbery scrotal mass.
a: Well circumscribed lesion with mixed, but predominately hypoechoicity. Separate to the underlying testes and epididymis.
b: Avid internal vascularity on Doppler colour flow.
c: TW2 coronal correlates with a well demarcated isointense lesion with internal mixed signal.
d: DWI b1400 restricted diffusion.
e: DCEI enhancement of the right scrotal mass.
References: Department of Radiology, University Hospital Plymouth NHS Trust, case courtesy of Dr Simon Freeman
Worrying features are the irregular hypoechogenicity and avid flow signal.


. These fascial layers are invested within a fibromuscular sac that contains the dartos muscle.")
 located on the distal portion of the spermatic cord.")
 soft tissue remnant projecting from the superior aspect of the testes (white arrow) with a small hydrocele (asterisk).
Image b: 12 year old presented with acute right scrotal pain. US grey scale shows an avascular extra-testicular mass with mixed echo texture (white arrow). No enhanced doppler flow.
The patient underwent surgery which confirmed a torted appendix testis")

 demonstrates 7.5 x 6.5cm echogenic fluid collection with dependant layering in keeping with recent haemorrhage. Image b: 32 days post-operative repeat US depicts a complex loculated extratesticular fluid collection with low echogenicity, septa and a fluid-debris level, in keeping with a chronic haematoma. Testicular vascularity was not compromised.")
. Extra-testicular slender floating echoes and thin internal septa (red arrows) favour pyocele. Patient was referred to urology, the final diagnosis of acute orchitis and an associated pyocele.")
 with posterior acoustic enhancement.")
 .
Spermatoceles are usually larger, irregular shaped cysts containing fine low-level internal echoes and occasionally separations as compared to epididymal cysts.")
.
No vascularity demonstrated on colour Doppler")
.
Appearances are typical of a scrotal calculi")
.
Note the separate normal appearance of the testes (asterisk)")
 smooth paratesticular ovid lesion with mild hyper-echogencity (arrrow) compared to the epididymal head. Normal testis (asterisk).
No significant colour Doppler vascularity
Absence of serum tumour markers.")
 in close association with the tunica vaginalis (arrows). Posterior shadowing suggests dense fibrotic content. Diffuse plaque like thickening of capsule.")


. Avascular on doppler Fluid collection communicates with the peritoneum at the internal inguinal ring, but not with the tunica vaginalis If it does not spontaneously regress, elective surgery is useful to prevent an acquired indirect hernia.")
 reaching up to the right scrotum (blue arrow)")




. The inner aspect of the scrotal wall (asterisk) is covered by the tunica albuginea (red arrow). The epididymal body (red star) is coarser in echotexture compared to the testes.")