A) IATROGENIC OR TRAUMA-RELATED BREAST LESIONS
a. Fat necrosis
Fat necrosis is a benign process due to previous trauma or surgery.
Clinical presentation is extremely variable; there may be asymptomatic or palpable masses that can be firm and fixed,
even with cutaneous changes.
Typical imaging findings are oil cysts with rim calcification on mammography.
However,
it may appear as a spiculated or irregular mass or asymmetry.
US findings spectrum is also variable.
US can show an irregular hypoechoic mass,
complex cystic and solid masses.
MRI may show high signal on T1WI and T2WI show low signal with fat suppression.
Therefore,
the best imaging tool is mammography,
where calcification pattern may help to reach the proper diagnosis.
However,
fat necrosis may overlap with malignant lesions,
so history of trauma or surgery must be taken into account.
Principal differential diagnosis includes fat-containing lesions (lipoma,
fibroadenolipoma,
galactocele) and cancer,
where biopsy must be performed if there is any doubt.

Fig. 1: A 50-year-old woman came for the first time to our hospital with history of breast cancer treated with surgery and radiotherapy in other hospital. A, B. Mammography of the left breast shows a spiculated nodule with skin thickening and retraction.
C. US findings show intense shadowing mass. Fat necrosis was confirmed in the biopsy.
References: Department of Radiology, Hospital Clínico San Carlos, Madrid/ES.
B) INFLAMMATION
a. Mastitis and abscess
Mastitis is a focal or diffuse breast infection which can be seen in lactating or nonlactating women.
The clinical signs of acute mastitis include redness,
heat,
and pain which help to diagnosis as well as the response to antibiotics.
Chronic mastitis is more frequent in non-puerperal state and presents clinically with a breast lump,
asymmetric breast thickening and can have axillary lymphadenopathy.
Mammography can show focal/diffuse skin thickening or an ill-defined focal asymmetry.
On ultrasound can be found skin thickening,
hyperechogenicity of fat,
dilated ducts or lymphatics.
An abscess can also be seen.
MRI can show focal or diffuse skin thickening,
thick-walled focal mass with different degree of contrast enhancement,
ductal enhancement,
and lymphadenopathy.
These image findings are non-specific and can be found in inflammatory or locally advanced breast cancer.
For this reason,
if there is no response or incomplete response to antibiotic treatment within two weeks,
malignancy should be considered.

Fig. 2: Chronic mastitis. A, B. Craniocaudal and mediolateral oblique mammograms show a hyperdense mass with an irregular shape and a spiculated margin. There are nipple retraction and enlarged axillary lymph nodes.
C. On ultrasound it corresponds with an irregular hypoechoic mass with nipple retraction.
References: Department of Radiology, Hospital Clínico San Carlos, Madrid/ES.

Fig. 3: Mastitis with breast abscess. A 26-year-old patient who was diagnosed with left breast mastitis without response to antibiotic treatment. Inflammatory breast cancer (IBC) was suspected, she underwent multiples biopsies that were negative for malignancy. A. Craniocaudal bilateral mammograms show diffuse left breast enlargement, diffuse increased density and skin thickening. B. Ultrasound image shows an irregular hypoechoic mass with skin thickening. C, D. MRI Axial T1WI and T2WI. The images show diffuse left breast enlargement with a heterogeneous mass that occupies almost the whole breast, thickening and retraction of the skin. E, F. Sagittal subtracted, and axial postcontrast MRI shows a heterogeneous and rim-enhancing mass in the left breast, thickening and enhancing of the skin and multiple enlarged axillary lymph nodes.
References: Department of Radiology, Hospital Clínico San Carlos, Madrid/ES.

Fig. 4: Non-specific chronic mastitis and acute mastitis.A 38-year-old patient with a palpable tumor on the upper inner quadrant of her left breast with high clinical suspicion for breast carcinoma. She underwent a core needle biopsy and excisional biopsy that were negative for malignancy. A. Axial T1WI shows an irregular mass on the upper inner quadrant of the left breast with thickening of the skin. B. The lesion shows high signal on diffusion-weighted image. C. Axial postcontrast MRI shows irregular enhancing mass with subtle skin retraction, thickening, and enhancement of the skin. D. Sagittal subtracted postcontrast MRI shows an irregular enhancing mass that contacts the skin. E, F. kinetic analysis (curves). Type 2 curve with a rapid initial rise followed by a plateau in the late phase.
References: Department of Radiology, Hospital Clínico San Carlos, Madrid/ES.
b. Idiopathic granulomatous mastitis
Idiopathic granulomatous mastitis is a chronic inflammatory breast entity caused by noncaseating granulomatous inflammation centered on lobules.
The most frequent clinical finding is a unilateral tender breast mass that may form tracks to skin-draining purulent content.
This disease usually affects young women where lactation may be a trigger.
The most common imaging findings are asymmetry and irregular masses and skin thickening at mammography.
Ultrasound findings include irregular tubular hypoechoic lesions.
MR imaging may show rim enhancing masses.
It is a diagnosis of exclusion when there is no response to antibiotic therapy,
and other causes of granulomatous inflammation have been discarded.

Fig. 5: Idiopathic granulomatous mastitis. A. Diagnostic mammography show an asymmetrically increased density in the outer quadrants of the right breast. B. US findings show hypervascularity and multiple hypoechoic linear tracks with surrounding inflammatory changes C. MRI, postcontrast sequences. there was an enhancing mass in the right breast and thickening of the skin D) MRI Maximum intensity projection.
References: Department of Radiology, Hospital Clínico San Carlos, Madrid/ES.
c. Diabetic mastopathy
Diabetic mastopathy is a rare illness typically described in type I diabetes.
It can be seen in both genders,
most often in females with longstanding diabetes and 40-50 years old.
Clinical features are large,
palpable and hard masses,
usually painless,
multiple and bilateral.
At mammography,
breasts are often dense with ill-defined masses.
Ultrasonographic findings are hypoechoic masses with posterior acoustic shadowing.
MRI findings are not specific,
mimicking carcinoma.
Needle core biopsy is necessary,
showing dense collagenous stroma and increased stromal spindle cells,
and perivascular lymphocytic infiltrate around ducts.

Fig. 6: Diabetic mastopathy. Woman with long-standing insulin-dependent diabetes A. Diagnostic mammography. An asymmetrically increased density in the outer quadrants of the right breast with small round calcifications. B. MRI. Heterogenous enhancing mass with spiculated margin. C, D. Maximum intensity projections. There is also a non-mass enhancement with satellite nodules.
References: Department of Radiology, Hospital Clínico San Carlos, Madrid/ES.
d. Sarcoidosis
Sarcoidosis is a multisystem chronic inflammatory disease that mainly affects middle-aged women (3rd-4th decade).
It affects multiple organs; mediastinal lymph nodes and lungs are the most frequently affected.
The mammary affectation in patients with known sarcoidosis is inferior to 1%,
and it is exceptional the primary mammary affectation.
The diagnosis of breast sarcoidosis is difficult,
especially when there is no known systemic involvement since findings are very nonspecific and they simulate clinical and radiological malignancy.
Due to this,
it is necessary to carry out a biopsy to be able to demonstrate noncaseating epithelioid granulomas and to rule out malignancy and other causes of a granulomatous process.
The most frequent clinical breast manifestation is a palpable mass with lymph node involvement in a woman.
Radiologically,
the most frequent findings are irregular,
spiculated or poorly defined masses on mammography and hypoechoic irregular masses on ultrasound.
MRI can present suspicious findings of malignancy such as masses with heterogeneous signal and irregular contours and rapid initial rise enhancement with washout in the delayed phase.

Fig. 7: Primary sarcoidosis of the breast. A 69-year-old-female that presented with painless and palpable bilateral masses without history of systemic sarcoidosis. A. Bilateral CC mammography showed bilateral indistinct and oval-shaped masses. B. Ultrasonography showed multiple hypoechoic, oval and not-circumscribed masses surrounded by an echogenic rim C,D. MRI shows bilateral irregular and enhancing nodules with a rapid initial rise followed by a plateau in the late phase.
References: Department of Radiology, Hospital Clínico San Carlos, Madrid/ES.
C) NON-PROLIFERATIVE AND PROLIFERATIVE DISEASES
a. Fibrocystic change of the breast (FC)
FC is a common benign breast condition that may appear focal,
regional or diffuse.
FC includes a wide variety of benign non-proliferative and proliferative histology (Stromal fibrosis,
adenosis,
cysts,
apocrine metaplasia,
and epithelial proliferation of various degrees) but without a dominant distinctive process.
It is thought to be caused by the response of the breast tissue to the estrogen and progesterone levels.
Most of the patients with FC of the breast show typical clinical symptoms and benign imaging features but sometimes they can show a focal lesion mimicking a tumor in clinical and imaging studies.
On mammography,
FC can mimic breast cancer when shows a mass or asymmetric density.
On ultrasound when it is presented as a complex cystic and solid mass or masses with acoustic shadowing.
FC has a broad spectrum of morphologic and kinetic features on MRI but usually presents as a mass or as a non-mass regional enhancing lesion with benign kinetics.
However sometimes can show morphologic or enhancement kinetics features of malignant breast lesions.

Fig. 8: Fibrocystic changes (Stromal fibrosis and adenosis). A 44-year-old woman with family history of breast cancer and a palpable mass in the right breast. A. Craniocaudal mammogram shows a focal asymmetric density in the upper inner quadrant of the right breast.
B. ultrasound shows an area of heterogeneous echogenicity and acoustic shadowing without a mass. C,D MRI shows an irregular mass that is hypointense on T2WI with heterogeneous patched enhancement areas and areas without enhancement. E,F. Kinetic analysis shows a rapid initial rise followed by a plateau in the delayed phase (type 2 curve).
References: Department of Radiology, Hospital Clínico San Carlos, Madrid/ES.

Fig. 9: Fibrocystic changes (Fibroadenoma, sclerosing adenosis and a focus of usual ductal hyperplasia without atypia). A 24-year-old woman with palpable mass and retraction of the nipple that underwent multiple biopsies that were negative for malignancy. Finally, due to the radio-pathological discordance, surgery was performed.
A. Bilateral OML mammograms: Asymmetry of size and an asymmetric focal density in the upper quadrants of left breast, distortion and nipple retraction. B. US: Multiple irregulars, uncircumscribed, and hypoechoic masses with posterior acoustic shadowing.
C. Sagittal T2 MRI shows distortion in the upper quadrants of left breast with nipple retraction.
D, E. (Sagittal postcontrast wT1 fat-suppressed MRI )and F, G (axial postcontrast T1 fat-suppressed MRI) show an area of nonmasslike enhancement in the upper quadrants with segmental distribution and nipple retraction.
References: Department of Radiology, Hospital Clínico San Carlos, Madrid/ES.
b. Sclerosing adenosis
Sclerosing adenosis (SA) is a proliferative lesion of the terminal duct lobular unit with an increased number of acini that may produce a mass or become surrounded by stromal sclerosis.
These lesions almost exclusively affect premenopausal women and is believed to be a response to an abnormal hormonal environment.
SA is found in 12% and 5-7% of biopsies from noncancerous and cancerous breasts respectively.
SA can coexist with other types of benign lesions as well as malignancies but also can be observed as a unique entity.
SA may mimic breast cancer clinically and radiographically because it usually presents as a firm,
palpable mass or as suspicious findings on imaging.
On mammography,
SA may show diffuse or clustered microcalcifications,
mass with irregular shape or spiculated borders,
asymmetric focal density,
and architectural distortion.
On ultrasound may present as an ill-defined mass with acoustic shadowing or a circumscribed mass with a well-defined,
microlobulated or irregular margin. On MRI SA can show an enhancing mass with irregular shape,
spiculated margin,
rim enhancement and heterogeneous internal pattern and also a non-mass enhancing lesion with segmental or linear distribution.
Both mass and non-mass enhancing lesions may show rapid initial contrast uptake and wash-out or plateau dynamic curves.

Fig. 10: Sclerosing adenosis. A, B, C. CC, OML mammography and ultrasound show an irregular circumscribed mass with fine pleomorphic calcifications.
D. Lateral mammography of the left breast shows fine pleomorphic calcifications with segmental distribution.
References: Department of Radiology, Hospital Clínico San Carlos, Madrid/ES.
c. Stromal fibrosis
Stromal fibrosis (SF) is a benign histopathological diagnosis characterized by obliteration of mammary ducts and lobules and proliferation of fibrous stroma with atrophy.
SF is a common finding on percutaneous biopsy with an incidence from 2-9%.
The pathogenesis is unknown,
but it is more frequent in premenopausal women which favors a hormonal role.
SF may present as a palpable mass or more frequent as a clinically occult and image-detected abnormality.
SF has no typical radiological findings with a wide spectrum of imaging features.
On mammography,
we can find ill-defined or spiculated masses and architectural distortion.
Suspicious microcalcifications have not been described as a feature of SF.
On ultrasound,
it can show focal architectural distortions,
irregular masses or acoustical shadowing. The most common MRI features are a round or oval shape,
irregular or spiculated margins,
rapid or medium rate of initial contrast uptake and plateau or washout curves.
It has been observed that SF can occur as a desmoplastic response to malignancy and as a result a proportion of percutaneous biopsies that show SF may be owing to undersampling of an adjacent malignancy.
To avoid this histopathology diagnosis of SF should be considered concordant if accurate targeting is confirmed and in the absence of imaging features that are suspicious of malignancy.
The ratio of radio-pathological discordance is between 0-6% in the literature,
and the false-negative rate is 2% for this reason,
concordant cases of SF should have a short-term follow-up.

Fig. 11: Stromal fibrosis. A 76-year-old woman. Screening mammogram. A. Right craniocaudal mammography. B. Tomosynthesis shows a subtle distortion in the upper inner quadrant. C. Ultrasound shows the distortion without other findings associated.
References: Department of Radiology, Hospital Clínico San Carlos, Madrid/ES.

Fig. 12: Stromal fibrosis. A. Ultrasound shows an irregular uncircumscribed mass. B. Ultrasound shows an area of acoustical shadowing.
References: Department of Radiology, Hospital Clínico San Carlos, Madrid/ES.
E) BENIGN BREAST TUMORS
a. Fibroadenoma
Fibroadenoma is a benign fibroepithelial tumor that develops in the lobules at the ends of mammary gland ducts and is composed of the epithelium and stroma.
Approximately 15% of fibroadenomas contain other proliferative changes of the breast,
such as sclerosing adenosis,
adenosis,
and epithelial duct hyperplasia.
These fibroadenomas are called complex fibroadenomas.
Fibroadenomas are the most commonly found breast tumors in adolescent girls and Young women.
Fibroadenoma is usually a mass with benign findings,
but 25% can show suspicious findings including irregular shape and contour and calcifications on mammography and irregular or microlobulated margins with posterior acoustic shadowing on ultrasound.
The MRI appearance of fibroadenomas is variable depending on the cellularity.
They usually have low signal on T1W and on T2WI the signal intensity may be very low (sclerotic fibroadenomas) or very high (myxomatous fibroadenomas).
The degree of contrast enhancement is variable with rapidly enhance in myxomatous lesions and minimally enhance in sclerotic fibroadenomas.
In 39-64% of fibroadenomas may be identified internal septations on either the T2-weighted or the postcontrast images.
However,
fibroadenomas may show suspicious findings like indistinct margins,
peripheral enhancement,
fast enhancement,
and washout.
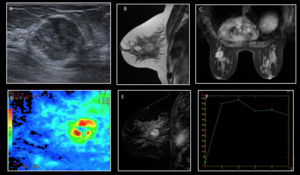
Fig. 13: Fibroadenoma. A 46-year-old woman with a palpable mass in the outers quadrants of the left breast. A. Ultrasound. Irregularly shaped mass with non-circumscribed margins. A core needle biopsy was done with a result of benignity. B. T2. Mass with irregular shape and margins. C, D. Postcontrast sequences. Irregularly shaped mass with heterogeneous enhancement pattern. E,F. Kinetic analysis (curves). Type 3 curve with a rapid initial rise followed by washout in the delayed phase.
References: Department of Radiology, Hospital Clínico San Carlos, Madrid/ES.



 was suspected, she underwent multiples biopsies that were negative for malignancy. A. Craniocaudal bilateral mammograms show diffuse left breast enlargement, diffuse increased density and skin thickening. B. Ultrasound image shows an irregular hypoechoic mass with skin thickening. C, D. MRI Axial T1WI and T2WI. The images show diffuse left breast enlargement with a heterogeneous mass that occupies almost the whole breast, thickening and retraction of the skin. E, F. Sagittal subtracted, and axial postcontrast MRI shows a heterogeneous and rim-enhancing mass in the left breast, thickening and enhancing of the skin and multiple enlarged axillary lymph nodes.
References: Department of Radiology, Hospital Clínico San Carlos, Madrid/ES.")
. Type 2 curve with a rapid initial rise followed by a plateau in the late phase. References: Department of Radiology, Hospital Clínico San Carlos, Madrid/ES.")
 MRI Maximum intensity projection. References: Department of Radiology, Hospital Clínico San Carlos, Madrid/ES.")


. A 44-year-old woman with family history of breast cancer and a palpable mass in the right breast. A. Craniocaudal mammogram shows a focal asymmetric density in the upper inner quadrant of the right breast.
B. ultrasound shows an area of heterogeneous echogenicity and acoustic shadowing without a mass. C,D MRI shows an irregular mass that is hypointense on T2WI with heterogeneous patched enhancement areas and areas without enhancement. E,F. Kinetic analysis shows a rapid initial rise followed by a plateau in the delayed phase (type 2 curve). References: Department of Radiology, Hospital Clínico San Carlos, Madrid/ES.")
. A 24-year-old woman with palpable mass and retraction of the nipple that underwent multiple biopsies that were negative for malignancy. Finally, due to the radio-pathological discordance, surgery was performed.
A. Bilateral OML mammograms: Asymmetry of size and an asymmetric focal density in the upper quadrants of left breast, distortion and nipple retraction. B. US: Multiple irregulars, uncircumscribed, and hypoechoic masses with posterior acoustic shadowing.
C. Sagittal T2 MRI shows distortion in the upper quadrants of left breast with nipple retraction.
D, E. (Sagittal postcontrast wT1 fat-suppressed MRI )and F, G (axial postcontrast T1 fat-suppressed MRI) show an area of nonmasslike enhancement in the upper quadrants with segmental distribution and nipple retraction.
References: Department of Radiology, Hospital Clínico San Carlos, Madrid/ES.")



. Type 3 curve with a rapid initial rise followed by washout in the delayed phase.
References: Department of Radiology, Hospital Clínico San Carlos, Madrid/ES.")