ANATOMY Fig. 1
It is a hollow muscular distensible organ situated in the base of the pelvis,
with extraperitoneal location,
only covered by peritoneum on the dome,
where the rectovesical recesses (men) and vesicouterine (women) are distinguished.
Arterial supply:
Vaculature from branches of the internal iliac artery
- Superior vesical artery: supplies blood to the upper part of the bladder.
- Blood in males,
this is supplemented by the Inferior vesical artery (lower part of the bladder)
- in females by the vaginal and uterine arteries (lower part of the bladder)
- In both sexes,
the obturator and inferior gluteal arteries also contribute small branches.
Venous drainage:
- Male: vesical and prostatic plexuses drain into the internal iliac veins
- Female: vesical and uterovaginal plexuses draining into the internal iliac vein
Lymphatic drainage:
- The lymphatic drainage of the superolateral aspect of the bladder is into the external iliac chain.
- The neck and body drain into the internal iliac,
sacral and common iliac nodes.
Innervation
The bladder receives motor innervation from both sympathetic fibers,
most of which arise from the superior and inferior hypogastricand nerves,
and from parasympathetic fibres,
which come from the pelvic splachinic nerves.
IMAGING TECHNIQUES
Computed Tomography Cystography
- Indirect,
using the excretory phase of the intravenous iodine contrast.
- Direct,
using 10% diluted iodine contrast (Plenigraf® or Visipaque®) through a Foley catheter
Ultrasonography
Safe and painless technique,
widely available in the emergency room
Urinary bladder anatomy is best assessed with this modality.
It should not exceed 3-5mm in thickness.
A partially distended bladder may overestimate the thickening of the bladder wall.
It also allows the analysis of the urinary bladder content (detritus,
blood,
urolithiasis),
the ureteric jets,
and the post-miccional residual volume in patients with bladder outlet obstruction.
Abdominal CT
- Without iodine contrast: detects urolithiasis,
dens content in the urinary bladder (blood,
pus…) or gas.
- With iodine contrast and acquisition on portal venous phase (80-100 sec): assesses bladder wall (thickening,
enhancing,…) and paravesical space.
CONGENITAL ANOMALIES
Congenital Urachal anomalies
Incomplete obliteration of the embryological connection between the bladder dome and the umbilicus. Approximately 1/5000 patients (male 3:1).
Classification:
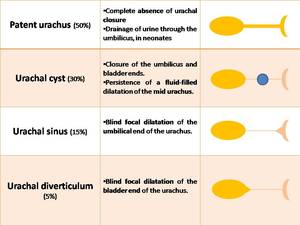
Fig. 2: Classification of congenital urachal anomalies: 4 types depending on the location and degree of obliteration
- Patent urachus
- Urachal cyst Fig. 3
- Urachal sinus
- Urachal diverticulum Fig. 3
Urinary stasis predispose to complication (infection,
litiasis) and over a long period the remnant may develop malignancy (adenocarcinoma).
Urachal anomalies may be visualized with ultrasound and cystography as a full-filled tubular structures following the expected trajectory of the median umbilical ligament,
in the space of Retzius.
CYSITITIS
Inflammation of the urinary bladder from any cause.
Bacterial cystitis
Infection of the bladder (Escherichia coli,
Staphylococcus saprophyctus, Klebsiella pneumoniae,
Proteus mirabilis).
It is a common condition especially in young women because of the shorter length and because the proximity of the urethra to the anus.
Risk factors: Active sexual life,
urogenital anomalies,
bladder obstruction,
foreign bodies.
Imaging techniques are not needed.
Thickened bladder wall,
+/- perivesical inflammatory changes.
Emphysematous cystitis Fig. 4
Rare form of complicated urinary tract infection. Patients present with variable clinical manifestations ranging from asymptomatic to severe sepsis.
Etiology:Escherichia coli,Enterobacter aerogenes, Klebsiella pneumoniae or Candida
Risk factors: diabetes mellitus,
immunocompromised state,
chronic catheterization,
neurogenic bladder
Radiological features: diffuse bladder wall thickening with intramural or intraluminal gas.
Cystitis Cystica and Cystitis Glandularis
Common chronic reactive inflammatory disorders which occur in the setting of chronic irritation of the bladder mucosa (infection,
calculi,
pelvic lipomatosis,
tumors).
It results in urothelial metaplasia,
which proliferates into buds,
which grow down into the connective tissue beneath the epithelium in the lamina propria.
- Cystitis cystica,
the buds differentiate into cystic deposits.
CT-urogram: multiple small 2-5mm smooth walled rounded filling defects projecting into the lumen Fig. 5
- Cystitis glandularis,
they differentiate into globlet cells.
CT: hypervascular polypoid masses within the urinary bladder.
Chemotherapy-related Cystitis
-Intravesical Bacillus Calmette-Guérin instillation (BCG) Fig. 6
Intravesical therapy with BCG (live attenuated strain of Mycobacterium bovis) for non-muscle invasive bladder cancer.
Symptomatology:
- Mild: dysuria,
frequency,
hematuria,
self-limiting fever
- Severe: pneumonitis,
sepsis,
skin rash,
sepsis,
renal abscess,
pancytopenia
Radiological features: irregular bladder wall thickening with adjacent inflammatory changes.
Intraluminal gas in the excretory system.
-Hemorrhagic cystitis Fig. 7
Complication of alkylating therapy (cyclophosphamide,
ifosfamide) used in lymphoproliferative syndromes,
solid tumors,
autoimmune diseases and conditioning for bone marrow transplantation,
attributable to its active metabolite acrolein,
which causes chemical irritation of the bladder epithelium.
Symptomatology: Dysuria and hematuria,
even incoercible.
Radiological features:
- Acute phase: Focal or diffuse mural thickening with increase of the Doppler signal.
Decreased distension due to spasticity, intraluminal clots.
- Chronic phase: mural thickening due to fibrosis.
Radiation induced Cystitis Fig. 8
Radiation injury may result from external,
interstitial or intracavitary radiation therapy for bladder or other pelvic malignancy,
and the effects may be acute or delayed.
Symptomatology:
- Mild forms: dysuria,
urinary retention +/- hematuria (10%)
- Severe forms: Bladder necrosis,
incontinence,
fistulas
Radiological features:
- Acute (<3months): Hemorrhagic cystitis secondary to denudation of the urothelium.
Focal or diffuse irregular bladder wall thickening,
spasticity,
decreased distensibility.
Wall hypervascularity, bleeding vessels and intraluminal clots.
- Chronic: Obliterative endarteritis in the lamina propria,
followed by ischemic changes and interstitial fibrosis.
Small fibrosed bladder with mural thickening.
Fatty replacement of the pelvic musculature and the sacral bone marrow associated.
Complex fistulas may develop.
Include cystoscopy to rule out radioinduced tumors not visible by CT.
Cystitis secondary to Graft versus Host Disease (GVHD) Fig. 9
Complication that may occur after bone marrow or allogeneic stem cells transplant.
GVHD with bladder involvement is a very rare entity.
It can be acute (<3 months post-transplant) or chronic (> 100 days post-transplant).
Symptomatology: Cystitis + hematuria (absence of infection).
Other organic involvement associated with GVHD (intestinal,
cutaneous...)
Radiological features:Hemorrhagic cystitis with bladder wall thickening and hyperemia.
BLADDER CALCULI
Concretions of mineral salts within bladder lumen,
usually a mixture of oxalate and calcium phosphate.
Etiology: classified as migrant,
primary (idiopathic,
rare in developed countries) and secondary
- Stasis (70%): bladder outlet obstruction (cystocele,
diverticulum,
neurogenic bladder,
urethral stricture)
- Infection (Proteus mirabilis)
- Foreign bodies: Nidus for crystal growth (chronic catheterization,
stents)
Radiological features: most are radiopaque Fig. 10
BLADDER OUTLET OBSTRUCTION Fig. 4
Hypertrophy of urinary bladder wall secondary to urethra and/or bladder outlet obstruction.
Patients present with difficulty in urination,
retention and discomfort.
Radiographic features: thickened and trabeculated walls.
Bladder diverticulum may be associated.
BLADDER DIVERTICULUM
Saccular structures formed by herniation of the mucosa and the submucosa through the muscular wall.
May be associated with a range of complications due to stasis,
including infections,
bladder stones,
rupture and intra-diverticular transitional cell carcinoma.
Etiology:
- Congenital
- Acquired: secondary bladder outlet obstruction or bladder dysfunction
- Associated syndromes: Menkes,
Ehlers-Danlos,
Prune belly
BLADDER HERNIA
Protrusion of part of bladder through the abdominal wall or the pelvic floor.
More common on right side,
through the inguinal canal (70%) and femoral canal (27%). Urinary obstruction and bladder distension increase the risk of herniation.
Classification:
- Paraperitoneal: portion of parietal peritoneum herniates along with bladder
- Intraperitoneal: herniated partis surrounded completely covered by peritoneum
- Extraperitoneal: intact peritoneum,
not herniated
The majority are asymptomatic,
dysuria,
urgency,
nocturia,
hematuria.
CT: The bladder points towards the site of herniation "arrow sign".
VESICAL FISTULAS
Non anatomic communication between bladder and the skin or adjacent organs.
Entero-vesical fistula
Symptomatology: recurrent cystitis,
pneumaturia,
fecaluria
Types:
- Colovesical: diverticulitis>rectosigmoid adenocarcinoma> Crohn,
RT Fig. 11
- Rectovesical: Tumor or trauma
- Ileovesical: Crohn disease,
foreign bodies (bones,
Foley)
Radiological features: Gas in bladder.
Mural thickening of bladder and bowel.
Enteric contrast material and feces within bladder lumen.
Vesicocutaneous fistula Fig. 12
Symptomatology: recurrent cystitis,
pneumaturia,
leakage of urine from the fistula
Etiology
- Surgical complication or trauma
- At site of prior suprapubic cystostomy after catheter removal
- Rare after radiation therapy
Vesicovaginal/vesicouternie fistula Fig. 13
Symptomatology: Urine leakage through the vagina. Youssef syndrome: amenorrhea,
menuria +/- urinary incontinence.
Etiology
- Gynecological surgery (hysterectomy): the most frequent 75%
- Obstetric complication: after a caesarean section
- Trauma,
RT
Radiological features: Gas in the bladder.
Contrast-opacified urine in vagina or uterus.
BLADDER ISCHEMIA Fig. 14
Rare condition with a mortality over 60%.
Multiorganic failure and paravesical blood vessels embolization are the most important predisposing factors,
but it is also associated with bladder outlet obstruction,
thrombophlebitis,
transurethral resection and pelvic radiotherapy.
Radiological features: hypoenhancing wall thickening associated with paravesical inflammatory changes and spontaneous bladder rupture.
TUMORAL CONDITIONS Fig. 15
Urinary bladder cancer represents 4% of all cancers and it is more common in men.
It is not an emergent condition but radiologists should bear it in mind when looking for a cause of hematuria in a patient who comes to the emergency room.
Symptomatology: hematuria,
dysuria,
bladder outlet obstruction and rupture,
either spontaneous or secondary to biopsy or intravesical chemotherapy.
1)Epitelial subtype (95%)
-Transitional cell carcinoma (90%) associated with smoking,
cyclophosphamide and polycyclic aromatic hydrocarbons.
Radiological features: asymmetric wall thickening with papillary superficial or invasive growth.
Calcifications are rare (5%)
-Squamous (6-8%):
Associated with chronic irritation by Schistosoma haematobium,
urolithiasis or bladder catheters.
Radiological features: in plaque thickening typically at the trigone or lateral walls of the bladder wall.
-Adenocarcinoma (2%)
Associated with urachal remnant, post surgical bladder extrophy and glandular cystitis.
Radiological features: asymmetric or diffuse thickened wall with heterogeneous contrast-enhancement,
cystic degeneration and calcifications (70%),
frequently associated with carcinomatosis.
2)Mesenchymal tumors: intramural nodules difficult to detect by TC or conventional cystography.
-Leimioma
-Paraganglioma
-Neurofibroma
-Hemangioma
-Lipoma
3)Differential diagnosis of bladder cancer
-Inflammatory pseudotumor:
Soft-tissue mass secondary to recurrent infections,
trauma or surgery.
Radiological features:endovesical polip with heterogeneous contrast-enhancement,
necrotic degeneration and peripheral calcifications.
-Endometriosis:
More frequent in patients with deep endometriosis and prior pelvic surgery.
Radiological features: submucosal nodule in the posterior wall of the bladder,
with heterogenous density.
-IgG4-related retroperitoneal fibrosis: Fig. 16
Direct infiltration of the bladder wall from retroperitoneal fibrosis,
typically at the trigone,
associated with hydronephrosis.
Diffuse thickening of the bladder is extremely rare (IgG4 cystitis).
-Lymphoma
- Primary lymphoma Fig. 17 is extremely rare (0.2%) and appears as focal or diffuse thickening of the bladder wall,
without pelvic lymphadenopathies or hydronephrosis.
- Secondary lymphoma Fig. 18 appears as an heterogeneous bulky mass which encases vessels and ureters (figure 8 and 9)
-Metastases
Direct spread from pelvic tumors (endometrial or colon cancer) is more frequent that hematogenous spread (melanoma,
breast or gastric cancer).
TRAUMATIC CONDITIONS
Bladder rupture
- Spontaneous bladder rupture is a rare but serious condition (25% mortality rate).
It is associated with tuberculosis,
Schistosoma,
tubo-ovarian abscess but also in patients with bladder calculus,
outlet obstruction,
cancer or prior pelvic radiotherapy.
- Iatrogenic bladder rupture: rupture is associated with complicated urinary catheterization,
intraabdominal drainage catheters Fig. 19 ,
transurethral resection Fig. 20 ,
or suprapubic cystostomy Fig. 21 .
Clinically,
patients presents with hypogastric pain,
dysuria,
hematuria and fever.
Radiological features: an irregular thickened wall and contrast extravasation.
Typically,
it is located at the posterior wall in patients with prior radiotherapy or at the dome in patients with bladder outlet obstruction.
Blunt trauma
Urinary bladder is the most frequent organ affected in blunt traumas,
especially in pelvic trauma with lateral compression.
Clinically,
patients present with macroscopic hematuria (84-95%),
hypogastric pain,
fever and adynamic ileus.
It can be categorized in five types:
1)Contusion (type 1) Fig. 22
Partial rupture of the bladder mucosa.
It presents in patients with mild traumas,
usually asymptomatic.
Radiological features: it may appear as a mild focal thickening of the wall with paravesical inflammatory changes; although in most cases there are not significant findings.
It may be associated with small pelvic hematomas.
2)Intraperitoneal rupture (type 2)
It occurs when there is a compression of the lower abdomen in a patient with a distendend urinary bladder,
causing a sudden rise in the intraluminal pressure of the bladder and rupture of the dome,
which is covered by peritoneum.
So an injury at this site causes intraperitoneal extravasation. Surgical treatment is always necessary.
3)Interstitial rupture (type 3) Fig. 23
It is rare and is defined as an intramural or partial-thickness laceration with intact serosa.
Radiological features: intramural lenticular hematoma under the serosa.
4)Extraperitoneal rupture (type 4)
It is the most common type of bladder injury (80%).
Rupture of the anterolateral walls of the bladder. It is usually caused by penetrating trauma,
in blunt trauma is caused by direct laceration of the bladder by bone fragments from pelvic fracture.
- Simple (type 4A):Contrast extravasation is confined to the paravesical space "molar tooth sign"
- Complex (type 4B): Fig. 24 Contrast material extends beyond the perivesical space and may dissect into other fascial planes and spaces (hip,
tigh,
abdominal wall,
scrotum,
pararenal space).
5)Combined rupture (type 5)
Simultaneous intraperitoneal and extraperitoneal injury.
It is associated with high risk of vascular lesions.
Surgical treatment is always necessary.
At the emergency room,
CT is the most effective imaging technique.
Ultrasonography detects free liquid in pelvis (EcoFAST) and MR depicts contusions and interstitial hematomas better than CT.
In patients with pelvic blunt trauma,
it is also necessary to check vascular integrity,
pelvic fractures,
urethral fractures and hemoperitoneum.
Mild ruptures usually resolve without surgical treatment in 10-14 days.
Major ruptures has a high mortality (12-22%) and are associated with higher risk of fistulas,
abscess and bladder calculus.



 A 10-year-old boy with an uncomplicated urachal cyst (red star) localized in the midline of the anterior abdominal wall, between the umbilicus and the pubis, contiguous with the bladder dome.
B) A 84-year-old man with an uncomplicated vesico-urachal diverticulum (green arrow)")
. Simple-CT revealed distended urinary bladder with diffuse wall thickening, several bladder calculi (green arrow) and intraluminal gas (yellow arrow).")
. Biopsy was performed with the definitive diagnosis of Cystitis cystica.")
, intraluminal vesical gas bubbles (red arrow) and perivesical fat-strading (green arrow). Intravesical BCG instillation-related cystitis was suspected.")
 with endoluminal hyperattenuating material (red star) corresponding to blood clots, and perivesical fat-strading (green arrow). The findings were compatible with Haemorrhagic chemotherapy-related cystitis")
 CT images show chronic radiation changes: an abdnormal diffuse bladder wall thickening (yellow arrow), presacral space widening (red star) and fatty infiltration of sacral bone marrow (green arrow). B) The same patient presented to the emergency room two years later, with a severe hemorrhagic cystitis, confirmed on the angiography images (red arrows) requiring selective embolization of vesical arteries.")
 complicated by chronic GVHD. Emergency CT shows extensive bladder pneumatosis (yellow arrow) and diffuse mural thickening of the jejunum, colon and rectum (green arrow).")
 stone in the bladder (yellow arrow).")
, perirenal collection (red star), mural bladder thickening and feces within bladder lumen (yellow arrow). Note the fistulous tract between the posterior wall of urinary bladder and sigma (red arrow).")
, disruption of the pelvic fasciae (green arrow) and a fistulous tract (yellow arrow) to the bladder. Gas was seen within the bladder, and CT-cystogram confirmed a fistulous tract from bladder to the extraluminal collection.")
, peritoneal pelvic and subcutaneous fluid, pelvic and Retzius’s space gas (yellow arrow). Note the abnormal and irregular bladder thickening and the intravaginal fluid and blood debris (yellow star).
Delayed phase from CECT shows a fistulous tract between the posterior bladder wall and upper vagina (red arrow). There is subsequent filling of the vagina with contrast-opacified urine.")
 in a 73-year-old man with radiation induced cystitis history. The patient presented to the emergency room with severe abdominal pain and hemodynamic instability. Emergency CT images show an hypoenhancing wall thickening with intramural gas (green circle). Paravesical fluid is observed (yellow star )without contrast extravasation (yellow arrow).")
. The tumour extends along anterior paravesical space (red star) and posterior paravesical space invading prostate and seminal vesicles(yellow star). Note the right ureter infiltration with secondary hydronephrosis (yellow arrow).")
 Biopsy was congruent with IgG4- related retroperitoneal fibrosis.")
 that extents into the anterior muscular compartment of the thigh, through the left inguinal (yellow star). Notice the pathologic fracture of the pubis bone (yellow arrow) and the encasement of the external iliac artery (green arrow). Cytological analysis demonstrated a diffuse large B-cell lymphoma (DLBCL).")
 history who presented to the emergency room with macroscopic hematuria. Abdominopelvic CT shows irregular and heterogeneous wall thickening of the bladder (yellow arrow). PET-CT with 18F-FDG shows bladder-wall increased metabolic uptake. Biopsy specimen obtained by cystoscopy demonstrated bladder wall infiltration by DLBCL.")
. Excretory phase CT depicts an extravasation of contrast-opacified urine into the rectovesical recess (yellow star).")
.
Portal and excretory venous CT demonstrate a transmural erosion in the bladder dome (yellow arrow) and massive amount of intraperitoneal free fluid. Iatrogenic intraperitoneal urinary bladder perforation was suspected.")
 (yellow arrow).")
 in a 40-year-old man who was involved in a motor vehicle accident. Emergency CT shows hyperdense bladder wall thickening(red star) and anterior paravesical hematoma (yellow star)")
 in a 48-year-old man who was involved in a motor vehicle accident. Emergency CT shows a hypodense intramural lenticular hematoma under the bladder serosa (red star). Arterial phase CT angiographic images depict a jet of extravasated contrast material within the hematoma that increases in portal venous phase, corresponding to active bleeding (yellow arrow).")
 in a 45-year-old man who was involved in a motor vehicle accident.
CT cystogram shows irregular bladder wall thickening (green circle) with gas and fluid within the perivesical space. There is extraperitoneal perivesicular extravasation with the typical "molar tooth appearance" (yellow arrows)and contrast material extension into the left posterior pararenal space (red arrow).")