ECR 2019 / C-2645
Non-cavernous cranial dural arteriovenous fistulas: Imaging findings that suggest them and classification
Congress:
ECR 2019
Poster Number:
C-2645
Type:
Educational Exhibit
Keywords:
Fistula, Embolisation, MR-Angiography, CT-Angiography, Catheter arteriography, Neuroradiology brain, Interventional vascular
Authors:
C. CASADO PEREZ, J. García Prieto, M. D. C. CRUZ CONDE, R. CASTRO VALDES, L. Koren, A. Ramos Gonzalez, A. Hilario Barrio; Madrid/ES
DOI:
10.26044/ecr2019/C-2645

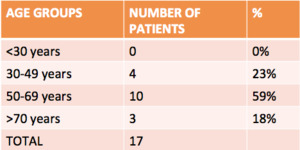
Fig. 2:
Distribution of the DAVF according to age groups.

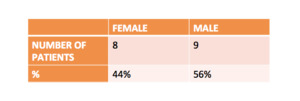
Fig. 3:
Distribution of the DAVF according the sex of the patients.

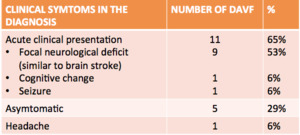
Fig. 4:
Distribution of the clinical symptoms of DAVF at the diagnosis.

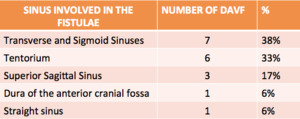
Fig. 5:
Distribution of the locations of the DAVF in our serie.

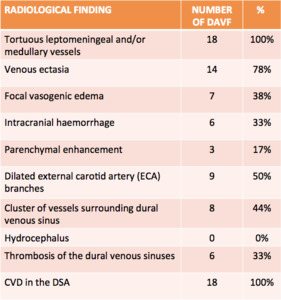
Fig. 6:
Distribution of the radiological finding of our patients at the diagnosis of...
 shows multiple temporo occipital microhemmorrhages (white arrows) and intraventricular haemmorrhage in the left occipital horn (yellow arrow). MR FLAIR (2) reveals an area of edema (white arrow) and CE-MRA 3DTOF (3) depicts tortuous vessels in the left hemisphere (arrowhead). DSA (4) confirms the presence of a dural fistulae with opacification of the left transverse sinus (blue arrow) and cortical veins in the arterial phase.")
Fig. 7:
73 YO male, arrived at the emengency department as a stroke code. MR...
 and CECT (2) shows a cerebellar hemorrhage (arrowhead) and dilated left cerebellar cortical veins (arrowhead). DSA (3 and 4) show a tentorial DAVF with arterial supply from both occipital arteries (red arrowhead), middle meningeal arteries (yellow arrowhead). Venous dreinage to cortical cerebellar veins (star). Cognard Grade IV.")
Fig. 8:
82 YO, woman, arrived at the emengency department with suspected stroke code....
 and MR Susceptibility Weighted Imaging (2), show intraparenchymal haemorraghes in the left occipital and temporal lobes (white arrows). CEMR 3DTOF (3) reveals leptomeningeal venous dilatation (blue arrow). DSA (4) demostrates a dural fistulae to the left transverse sinus (red arrow) with occlusion of transverse and stenosis of the sigmoid sinus, resulting in significant CVD.")
Fig. 9:
67 YO male, arrived at the emengency department with a severe confussional...
 shows a right intraparenchymal haemmorrhage in the right frontal lobe an a dilated vascular structure anterior to the hematoma (blue arrows). DSA (3) reveals dural fistulae of the anterior cranial fossa that is supplied by bilateral ethmoidal arteries and presents a venous drainage to a dilated cortical frontobasal vein which is opacified in the arterial phase (green arrow). DAVF Cognard type IV.")
Fig. 10:
53 YO male, arrived at the emengency department as a stroke code. CECT (1 and...
. NECT (1) and CECT (2) depicts a frontal parasagital left vascular structure (arrowhead) , there was not lesión related with traumatic injury. Two days later the DSA (3 and 4) reveals a anterior cranial fossa DVAF to a cortical vein (blue arrow) that drains in the anterior portion of the superior sagital sinus. The fistula presents venus ectasia. Notice the presence of another dural fistuale, also with CVD and venous dilatation, located in the inferior surface of the tentorium (green arrow). Both fistulaes were Cognard grade IV and asymptomatic.")
Fig. 11:
Male, 59 years old, ariived at he emengency department after a traumatic brain...
 shows mildly dilated right parieto-occipital cortical veins (yellow arrow) and a strongly dilated cortical vein (blue arrow) communicating to the superior sagittal sinus (DAVF with CVD). DSA (3 and 4) was performed, which shows a dural fistulae of the lateral wall of the sagittal sinus with arterial supply from ECA branches (MMA, superficial temporal and occipital arteries (green arrows)) and with CVD (yellow star on the foot of the vein, red arrowhead on the cortical vein)).")
Fig. 12:
63 YO male, arrived at the emengency department as stroke code. DAVF directly...
 (1) which has disappeared a week after the endovacular treatment (2). DAVF to the left posterior clinoid of the sella with arterial aference from meningohypophiseal trunk (3) (yellow arrowhead) and posterior branch of ascendig pharingeal artery (selective microcatheterism in 4 (red arrowhead in the foot of the vein)) and venous drainage toward the proximal portion of the right superior petrosal sinus (blue arrowhead in VR reconstruction in 5) associated with congestion of the brainstem via petrosal vein, lateral pontomedullary veins and cervical spinal drainage system (green arrowhead in 3 and in VR reconstruction in 5) and with suspected thrombosis of the distal portion of the superior petrosal sinus (white stars in 5).")
Fig. 13:
DAVF Cognard type V. T2 MR shows an area of edema in the spine bulb (blue...
 shows trombosis of the left transverse sinus (yellow arrow). MR Flair axial sequence (fig2) reveals an area of edema (red arrowheads) and CE MRA 3DTOF (fig 4) shows tortuous and dilated leptomeningeal veins due to DAVF(green arrow). DSA shows a dural fistulae in the transverse and sigmoid sinuses (blue arrow) whith opacification of the temporo-occipital veins in the arterial phase (CVD) grading II a+b in Cognard classification. DSA, venous embolization of previous DAVF with persistence of non-excluded segment of the transverse sinus (arrowhead) (5). ECA angiography (6) showing opacification of that segment (arrowhead) without significant CVR.")
Fig. 14:
72 YO, woman, arrived at the emengency department as a stroke code. DAVF of...