ECR 2019 / C-2655
Imaging hepatobiliary manifestations of parasitosis – hints leading to the differential diagnosis
Congress:
ECR 2019
Poster Number:
C-2655
Type:
Educational Exhibit
Keywords:
Liver, Ultrasound, CT, MR, Imaging sequences, Complications, Parasites, Abscess, Cysts
Authors:
L. B. Castelo David1, W. Schmitt2, P. Joao3, A. M. D. Costa4, A. S. C. C. Germano5; 1Amadora-Lisbon/PT, 2Amadora, Porto/PT, 3Lisboa/PT, 4Amadora/PT, 5Barcarena /PT
DOI:
10.26044/ecr2019/C-2655

Fig. 1:
Entamoeba hystolitica: Transmission route and life-cycle.
, contrast-enhanced ultrasound, and CT (axial and coronal) (images 3 and 4), showed 2 enormous, contiguous hepatic non-enhancing lesions (green stars), causing intra-hepatic bile duct dilatation and right diaphragm superior deviation.
Serology was positive for Entamoeba hystolitica.
Surgical drainage was performed and the patient was treated with metronidazole .
Budd-Chiari syndrome due to supra-hepatic veins’ thrombosis, and portal hypertension occurred as late complications.")
Fig. 2:
37 year-old male patient
Presented to the ER complaints of asthenia, anorexia,...
, contrast-enhanced ultrasound, and CT (axial and coronal) (images 3 and 4), showed 2 enormous, contiguous hepatic non-enhancing lesions (green stars), causing intra-hepatic bile duct dilatation and right diaphragm superior deviation.
Serology was positive for Entamoeba hystolitica.
Surgical drainage was performed and the patient was treated with metronidazole .
Budd-Chiari syndrome due to supra-hepatic veins’ thrombosis, and portal hypertension occurred as late complications.")
Fig. 3:
37 year-old male patient
Presented to the ER complaints of asthenia, anorexia,...
, contrast-enhanced ultrasound, and CT (axial and coronal) (images 3 and 4), showed 2 enormous, contiguous hepatic non-enhancing lesions (green stars), causing intra-hepatic bile duct dilatation and right diaphragm superior deviation.
Serology was positive for Entamoeba hystolitica.
Surgical drainage was performed and the patient was treated with metronidazole .
Budd-Chiari syndrome due to supra-hepatic veins’ thrombosis, and portal hypertension occurred as late complications.")
Fig. 4:
37 year-old male patient
Presented to the ER complaints of asthenia, anorexia,...

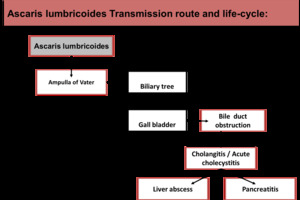
Fig. 5:
Ascaris lumbricoides: Transmission route and life-cycle
")
Fig. 6:
59 year-old male patient presented with diarrhoea, abdominal pain, and...
 (arrow) was incidentally found in a CT scan of a 50 year-old male, performed to stage a gastric carcinoma (star). No obstructive cause was found in the CT scan, nor in the subsequently performed MRI. The MRI (bottom images) revealed only a subtle ectasia of the left bile duct, with slightly restricted diffusion (arrows)
Due to the oncologic context, a metastatic possibility was considered and the left lobe of the liver was resected at the same time of the gastrectomy.
Pathology specimen (top right image, arrow) showed absence of neoplasia, together with hepatic granulomas and (impossible to characterise) degenerated parasitary structures.
Serology was positive only to Ascaris lumbricoides")
Fig. 7:
Segmental dilatation of a single left bile duct (top left image) (arrow) was...

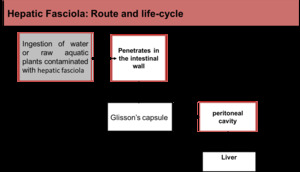
Fig. 8:
Fasciola hepatica: Transmission route and life-cycle
, plus diffuse peri-portal liver hypodensities (star). Lab tests were remarkable due to eosinophilia (8.3%), anaemia, and high-grade positive anti fasciola hepatica antibodies. Infection by Fasciola was considered the probable cause of the findings. She was treated with triclabendazol and 2 EC units. Follow-up CT (not shown) revealed complete resolution of the findings.")
Fig. 9:
A 73 year-old female, recently arrived from Cape Verde, presented to the ER...

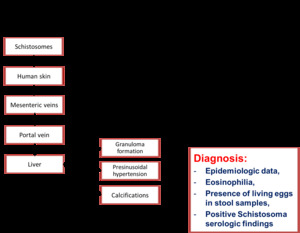
Fig. 11:
Shistosoma mansoni: Transmission route and life-cycle
 were pathognomonic of hepatic Schistosomiasis (arrows point to extensive periportal calcifications).")
Fig. 12:
A 17 year-old female living in the S. Tomé and Principe islands, presented ...
, and altered liver function tests.
Contrast-enhanced CT demonstrated sub-capsular hepatic collections, bile duct dilatations and heterogeneous liver, with multiple low-density lesions (arrows). A cholangiocarcinoma was considered as a possible diagnosis. Hepatic biopsies showed only inflammatory lymphocytic and eosinophilic infiltrates. Finally, a probable parasitary infection was considered. Serology revealed high levels of anti-fasciola antibodies.
A successful outcome was observed after treatment with triclabendazol, with improvement of symptoms and resolution of the imaging findings (bottom right image).")
Fig. 10:
A 77 year-old male, natural from Cape Verde, presented to the ER due to...
 were pathognomonic of hepatic Schistosomiasis (arrows point to extensive periportal calcifications).")
Fig. 13:
A 17 year-old female living in the S. Tomé and Principe islands, presented ...

Fig. 14:
Echinococcus granulosum: Transmission route and life-cycle
 (top image) (arrow); the other with detached membranes (CE3A) (bottom image) (double arrow)")
Fig. 15:
7 year-old girl presented to the ER with abdominal pain
Two liver hydatid...
.
A liver hydatid cyst was incidentally detected, CE type 2 (multivesicular)(arrow).")
Fig. 16:
Male patient, 75 years old, presenting with abdominal pain and nausea, caused...
, consistent with a hydatid cyst CE4.")
Fig. 17:
75 year-old male patient presented with abdominal pain, vomits, and a hard,...
 cystic mass, contiguous with the inferior liver border, better characterized by MR (axial T2 fat sat) (arrows). A hydatid cyst (CE2) was histologically confirmed.")
Fig. 18:
The patient described in the previous image also presented a voluminous complex...
 and US (bottom image, arrow)")
Fig. 19:
Incidentally found liver hydatid cyst CE 4. Heterogeneous matrix without...
")
Fig. 20:
57 year-old female;
Colon cancer staging
Incidentally found liver hydatid...
 (CT - top image; US - bottom image).")
Fig. 21:
78 year-old female;
Asymptomatic
Multiple calcified liver cysts, compatible...
 – anterior abdominal wall skin fistulization - US and CT (arrows)")
Fig. 22:
Complication of a left liver lobe hydatid cyst (CE3B/4) – anterior abdominal...
, best seen in ultrasound. There was also a liver image suggestive of a ruptured hydatid cyst (star).
Despite medical treatment, the patient died 2 days later.")
Fig. 23:
60 year-old female presented to the ER complaining of dyspnoea, abdominal pain,...